
Arthur Thomas Martella, MD & Bob Kiaii, MD
Coronary Artery Bypass Grafting (CABG)
Procedure Overview
A coronary artery bypass graft (CABG) is a heart bypass. The CABG procedure involves “bypassing” blood around blockages in the proximal coronary arteries. CABG surgery frequently involves harvesting blood vessels from the chest, arm or leg to be used as conduits in the bypass, followed by coronary anastomosis. The procedure can be performed On-pump or Off-pump.
INDICATIONS:
- Critical stenosis of the left main artery.
- Severe angina that does not respond to medication.
- Significant stenosis (> 60%) in at least one major coronary artery not amenable to PCI.
- Significant stenosis of all three major coronary arteries.
- Repeated angioplasty and repeated restenosis after angioplasty.
- Blockage in a graft created in previous surgery.
CONTRAINDICATIONS:
- Patients with coronary disease that’s amenable to PCI (stenting).
- High risk based on medical condition for open heart surgery (i.e., severe COPD, renal failure, obesity, age).
- CAD that is not amenable for bypassing.
- Patients without significant left anterior descending artery (LAD) disease.

Prep & Patient Positioning
Prep
- Femoral arterial access is sometimes obtained when radial artery monitoring is a concern.
Common patient positioning:
- The most common position used for cardiovascular procedures is the supine position. This type of position allows the best possible surgical access to the chest cavity.
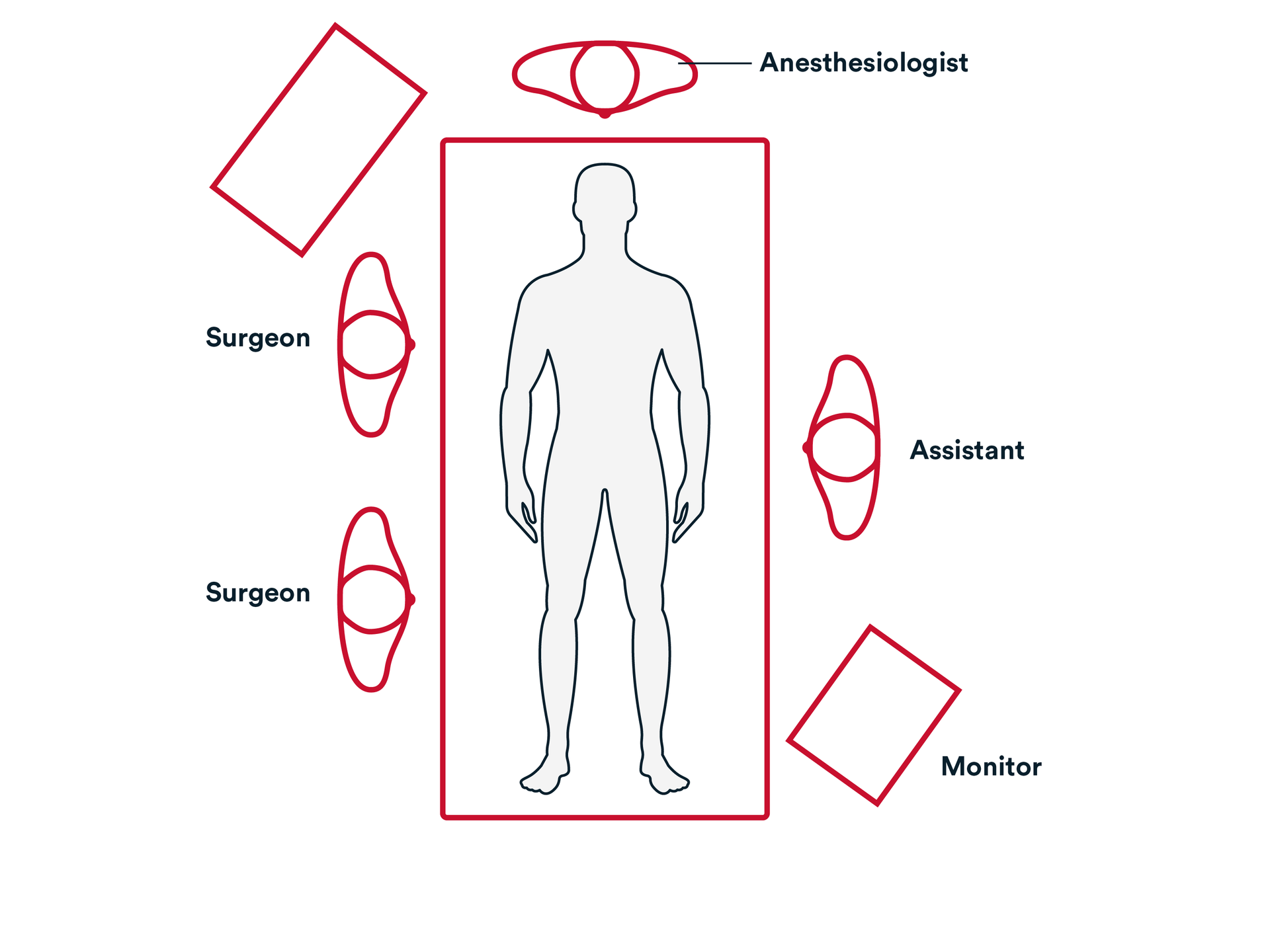
Common room setup
- The surgeon is almost always on the right side of the patient.
- Assistant on the left side.
- Bypass machine is usually close to the patient and can be on either side.
- Monitor that is positioned so the surgeon can see the hemodynamics during the procedure.
- Transesophageal echocardiogram machine is at the head of the patient.
Sternotomy:
- A sternal saw is used to open the entire length of the sternum from sternal notch to xyphoid process, staying in the midline of the sternum.

Sternotomy:
- Bleeding from the sternal marrow and periosteum is commonly controlled to avoid ongoing oozing throughout the procedure. A topical absorbable hemostat such as SURGICEL™ FIBRILLAR Absorbable Hemostat can be applied to the sternal edges and bolstered with a sterile drape and the retractors.
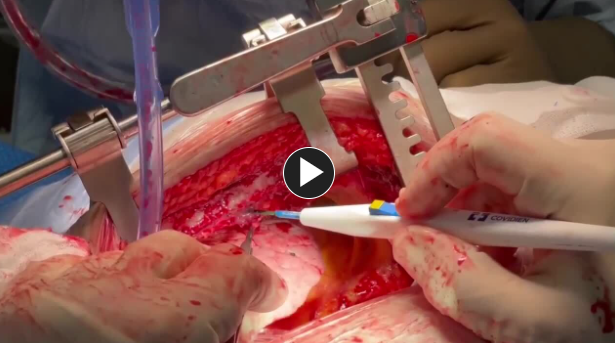
Dissection of the Left Internal Mammary Artery (LIMA):
- The left pleura is usually opened widely to further expose the artery which runs directly under the anterior chest wall.
Dissection of the Left Internal Mammary Artery (LIMA):
- LIMA is harvested using an energy device.
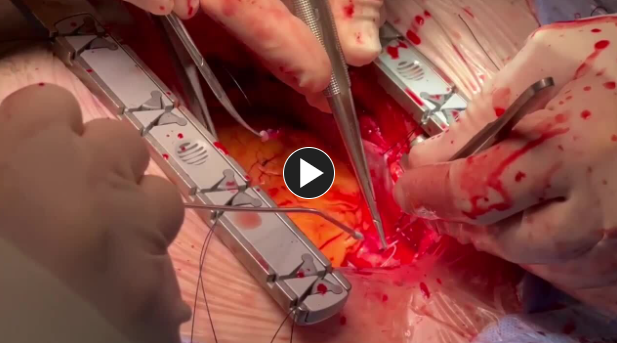
Suturing the Anastomosis:
- A general practice is starting at 3 o’clock on the right side of the conduit vessel, the suture is passed outside-in and then inside-out at the 3 o’clock location on the arterial target vessel.

Suturing the Anastomosis:
- Approximately three stitches are performed in the same manner at 2, 1, and 12 o’clock and then two more on the left side of that heel at 11 and 10 o’clock, followed by a parachuting technique in which the conduit is then brought down to the target vessel.
- NOTE: Alternatively, a U-stitch can be placed at the heel of the anastomosis without significant parachuting and both side of the suture are run.
- The anastomosis can then be completed by placing another six stitches, evenly spaced, utilizing the same technique, around the toe and back at the 3 o’clock position, where a final knot is placed on the side to secure the anastomosis.
- NOTE: Often, the conduit is distended with solution gently injected by the assistant while tying the sutures to avoid any constriction of the anastomosis. This also allows the surgeon to check for any leaks.

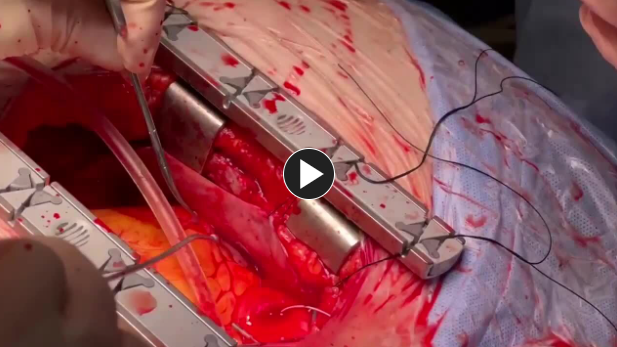
Proximal Anastomosis (single clamp technique):
- Generally, the vein graft is injected with vein solution and the length to the aorta is measured.

Proximal Anastomosis (single clamp technique):
que
- A circular hole is created using an aortic punch. The size of the aortic punch used depends on the size of the chosen conduit graft.
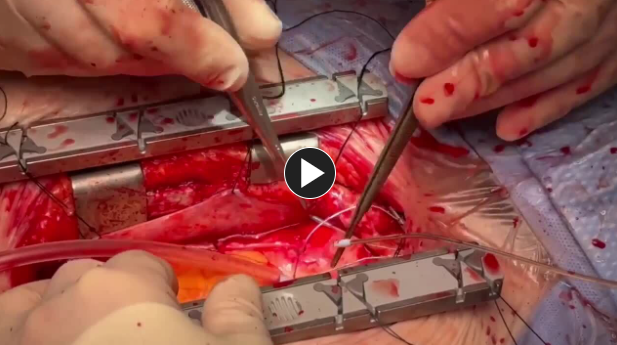
Proximal Anastomosis (single clamp technique):
- A running 5-0 or 6-0 polypropylene suture such as Prolene™ Polypropylene Suture, is commonly used for the proximal anastomosis; a running 6-0 or 7-0 polypropylene suture such as Prolene™ Polypropylene Suture, is commonly used for an arterial proximal anastomosis.
Proximal Anastomosis (single clamp technique):
- With the long axis of the graft aligned at an appropriate angle to the ascending aorta, anastomosis is completed generally with approximately 8- 10 stitches, ensuring that symmetry in the spacing between stitches is achieved for hemostasis.
3. Closure
- Confirm that there are no areas of active bleeding. Consider placing topical absorbable hemostat such as SURGICEL™ FIBRILLAR Absorbable Hemostat - on the sternal edges prior to closing the sternum to minimize oozing from the lower sternal table and to utilize its bactericidal affects.

- Sternal wires are placed starting from the top (manubrium), using Surgical stainless-steel suture.

- Tighten Steel Wires.


Access our on-demand Cardiovascular video library
Looking for more? Explore procedural videos and webinars from global experts
SuturED
SuturED consists of e-modules covering topics such as suturing techniques and the science of tissue management

