
George Crawford, MD
Inguinal Hernia Repair Open
Procedure Overview
Inguinal hernias can be categorized as direct, indirect, femoral.
Inguinal Hernia repair techniques fall under two categories: Tension and Tension Free.
Tension techniques suture the anterior abdominal walls or other structures together to recreate the inguinal canal. They are usually performed using an open procedure. This technique is often used where infection is a concern.
Tension free open repair options with mesh include Plug & Patch, Lichtenstein and Bilayer Connected Mesh Device.
INDICATIONS:
- The existence of an inguinal hernia has traditionally been considered sufficient reason for operative intervention.
- Surgical repair is recommended electively to avoid incarceration or strangulation. NOTE: reducible inguinal hernias can be safely observed in the elderly population with a sedentary lifestyle or high morbidity for surgery.
- Inguinal hernia repair has no absolute contraindications
(Back to the top)

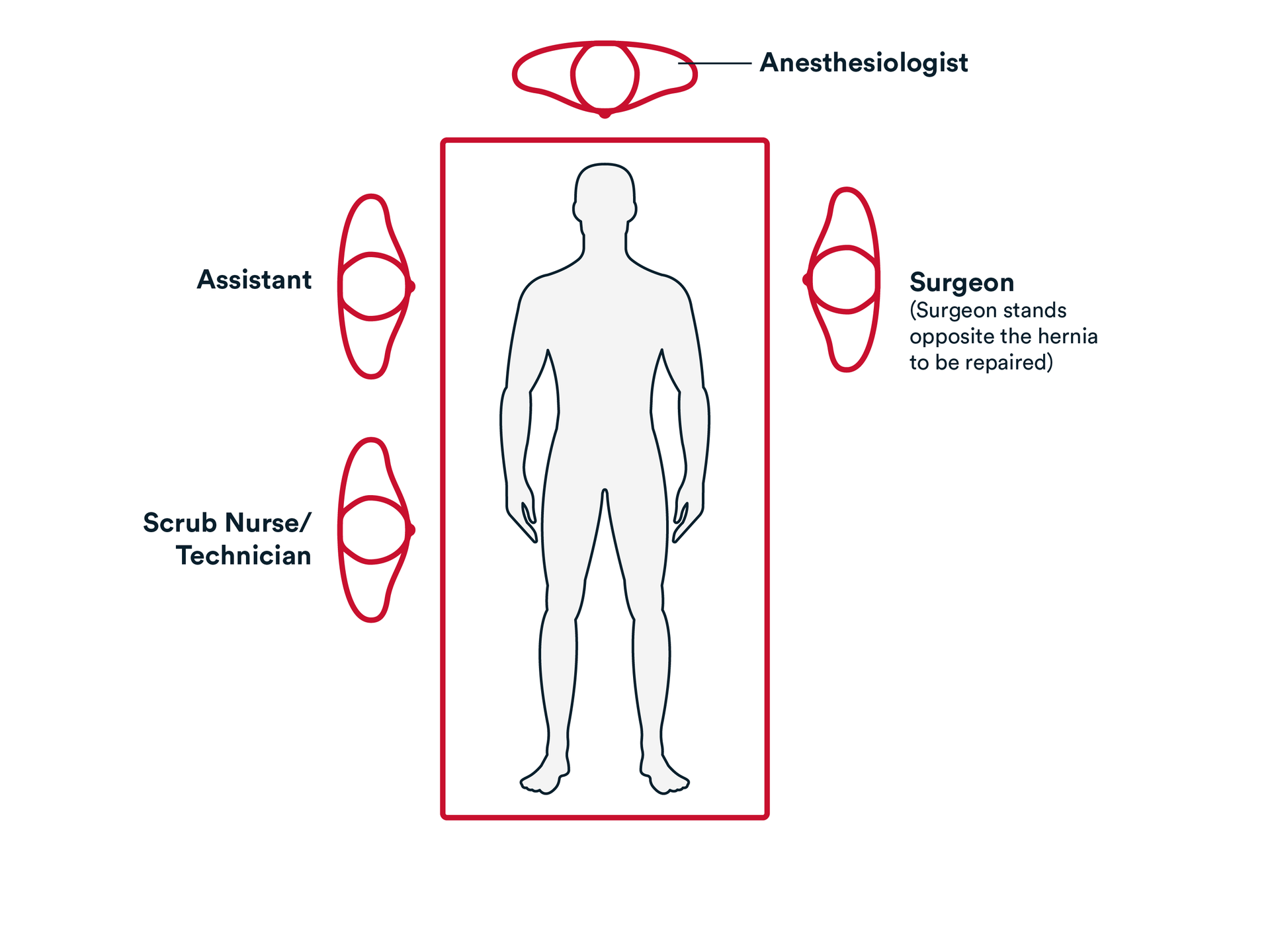
Prep & Patient Positioning
Common patient positioning:
- Open approach: The patient is positioned supine on the operating table. The correct surgical site is clipped free of hair and prepped in the standard sterile fashion.
Operative Steps
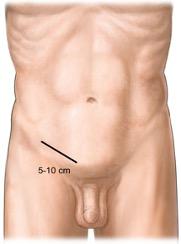
1. Access
- Generally, an incision is made over the inguinal canal, and it is carried down through the subcutaneous tissues.
- Scarpa’s fascia is then identified and incised. If needed, hemostasis may be obtained using electrocautery.
- The external oblique is identified. Typically, a small incision is made in the external oblique, and the Facia is separated and opened towards the external inguinal ring.
- The external oblique is generally retracted laterally to expose the inguinal canal, as well as the cord structures.
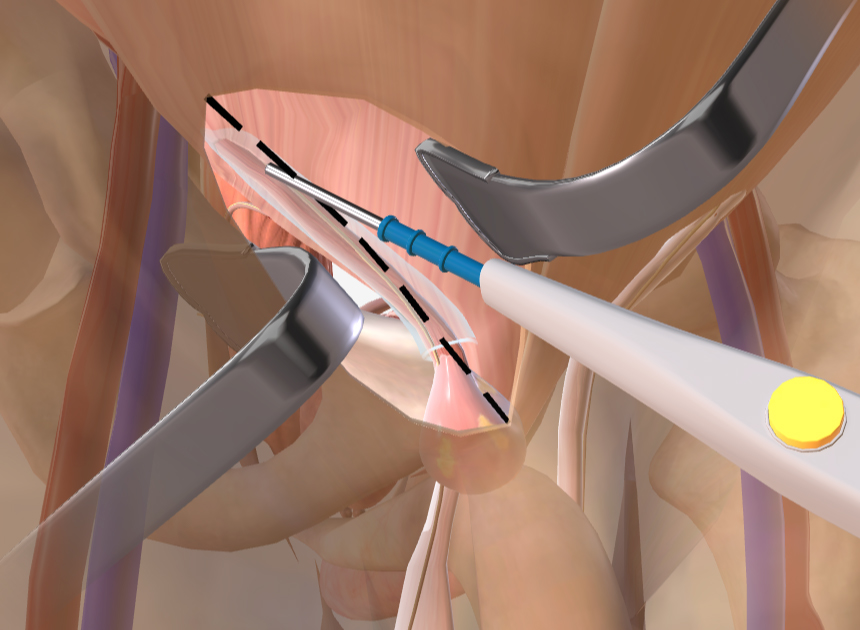
- The cord structures are dissected away from the pubic tubercle. Commonly, a Penrose drain is placed around the cord structures for retraction.
- Dissection on the cord structures is typically performed mediately to laterally to identify the indirect hernia sac.
3. Closure
- A size 0 suture, such as Coated VICRYL™ Plus Antibacterial suture is generally used to re-approximate the external oblique fascia in a running fashion.
- Size 3-0- suture, such as Coated VICRYL™ Plus Antibacterial suture is used to re-approximate Scarpa’s Fascia.
The wounds are closed using synthetic absorbable suture, such as MONOCRYL™ Plus Antibacterial suture, and a topical skin adhesive such as DERMABOND™ Mini Topical Skin Adhesive, or any appropriate dressing.
Additional resources

Access our on-demand Hernia video library
Looking for more? Explore procedural videos and webinars from global experts
HERNIAcademy
Offering comprehensive education about the treatment of inguinal and abdominal hernias

