
George Crawford, MD
Laparoscopic Appendectomy

Procedure Overview
Laparoscopic appendectomy is a minimally invasive surgical procedure to remove the vermiform appendix.
INDICATIONS:
- Appendicitis (Acute, Chronic, Gangrenous, Perforated, Suspected, or Uncomplicated)
- Incidental (during another procedure often due to injury or abnormal anatomy)
- Carcinoid tumors (in children and when confined to the tip of the appendix)
- Adenocarcinoma of the appendix requires a right colectomy

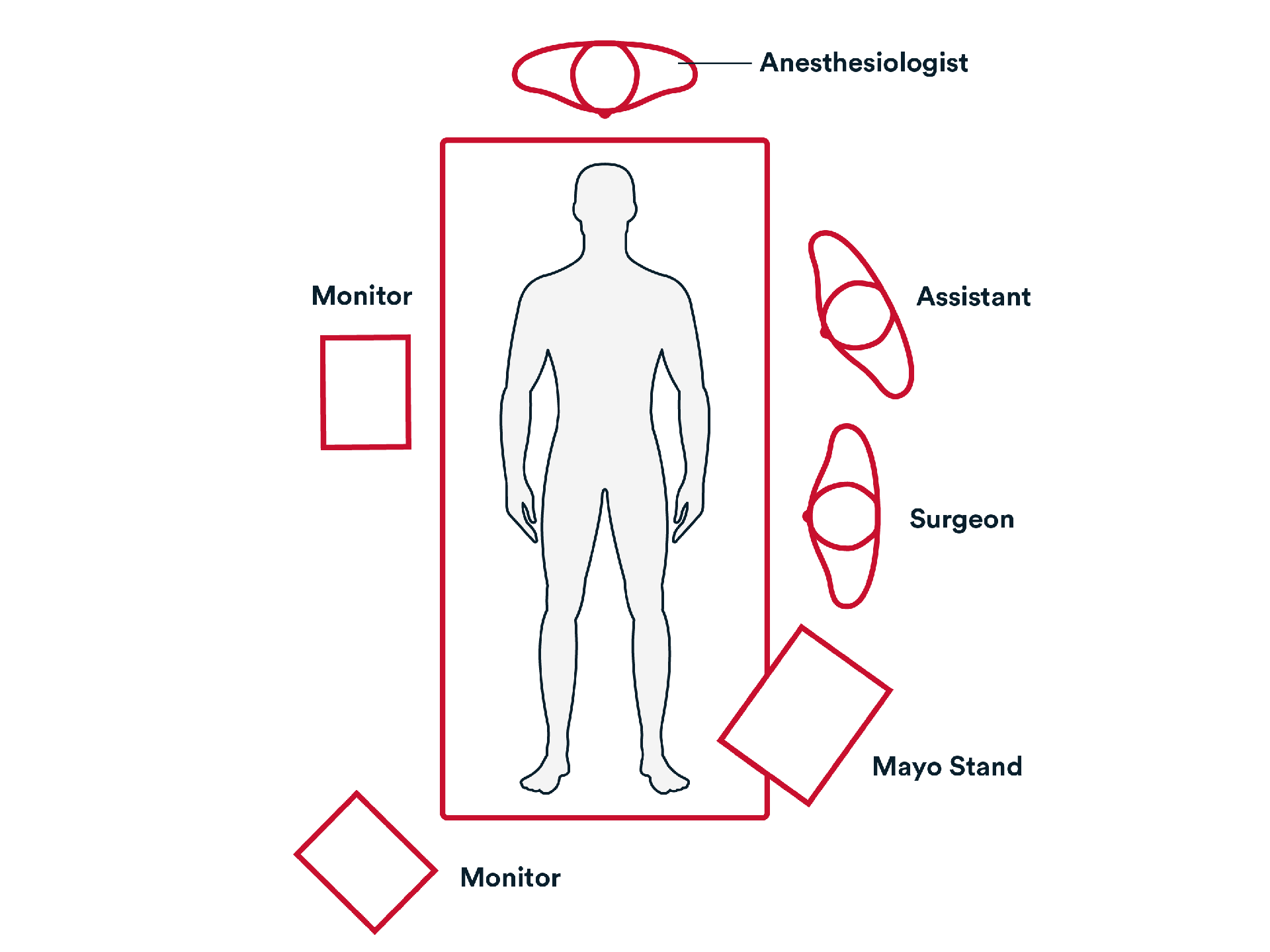
Common patient positioning:
- The patient is supine with both arms tucked at the sides. The operating surgeon and assistant stand on the patient's left.
Placing the patient with the left side down aids gravity in relocating the small bowel away from the appendiceal/cecal field of vision.
2. Repair
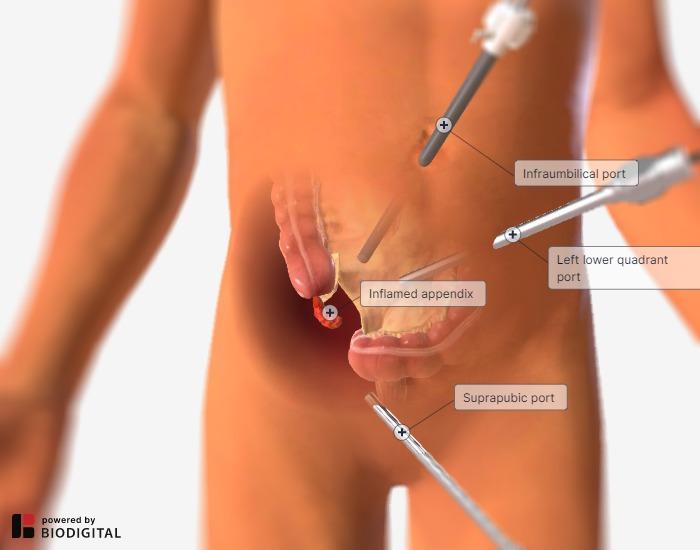
- The appendix is identified and retracted superiorly.

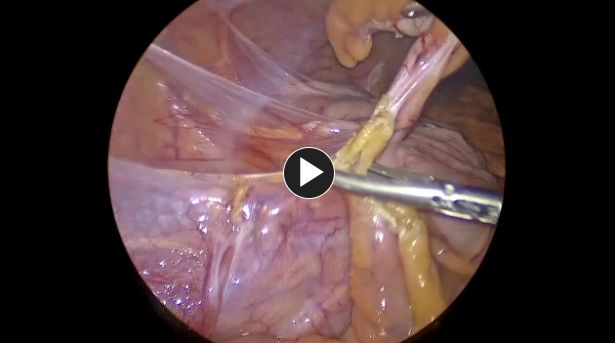
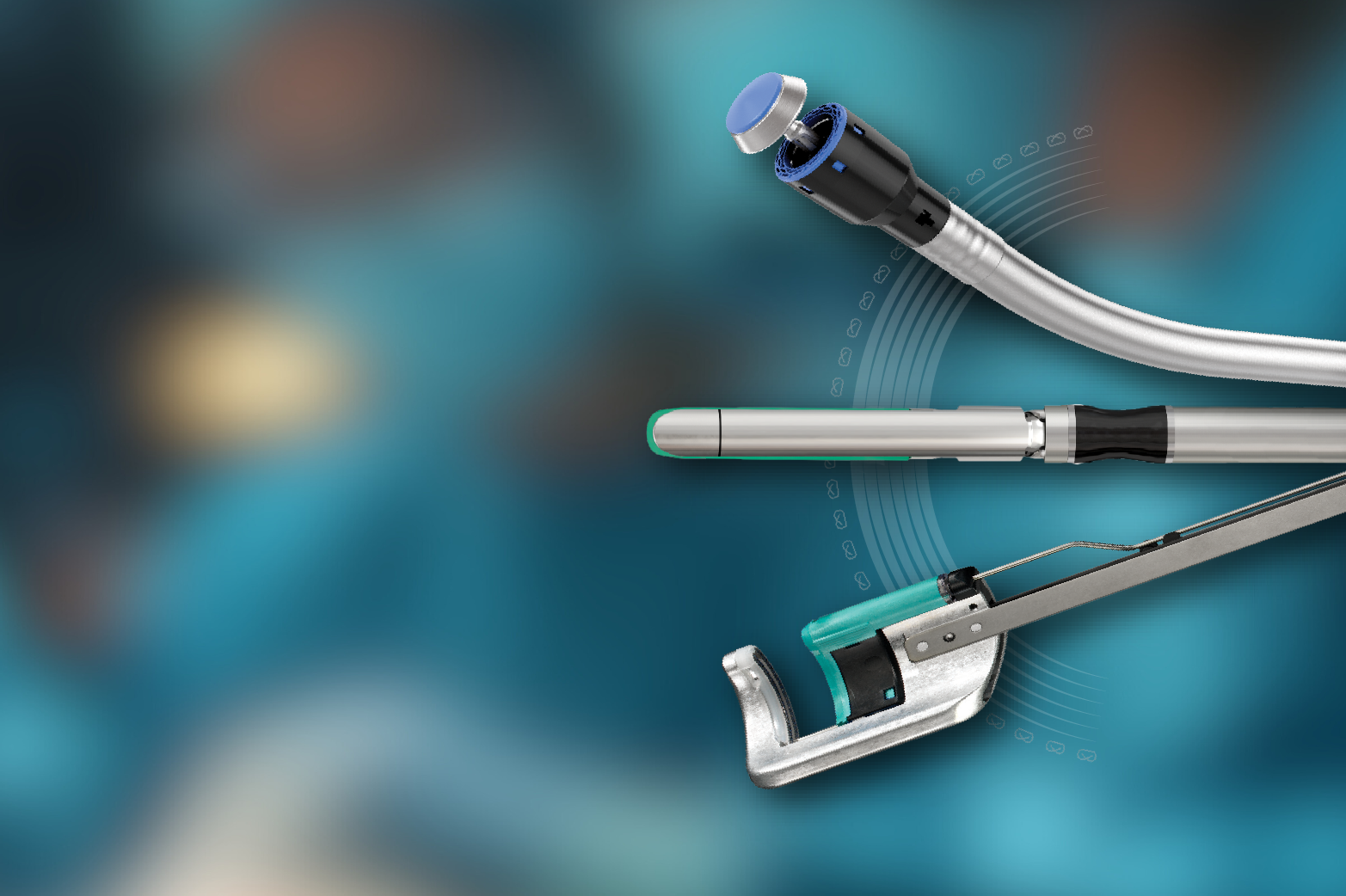
- The mesentery of the appendix is mobilized and transected using an energy device such as ENSEAL™ X1 Straight Jaw Tissue Sealer or HARMONIC™ 1100 shears.
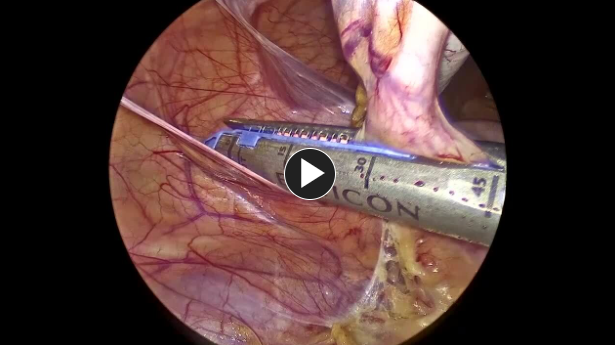
- An endoscopic stapler, such as ECHELON™ 3000 Stapler, is fired across the base of the appendix and cecum taking care to not leave an appendiceal stump.
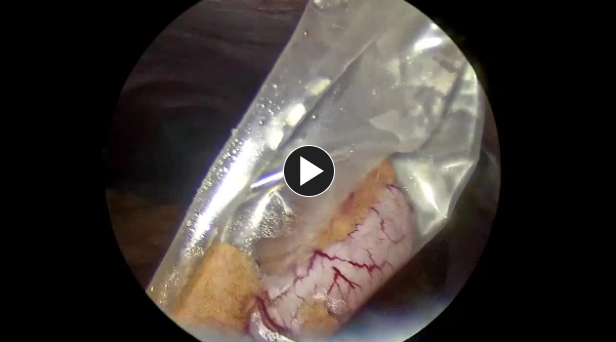
- The appendix is removed in the specimen retrieval bag through the 12 mm trocar site.
(Back to the top)
3. Closure
- A suture like a size 0 Vicryl™ Plus Antibacterial suture, is used to reapproximate the fascia of the umbilicus.
- The remaining trocars are removed. The wounds are closed using synthetic absorbable monofilament, such as Monocryl™ Plus Antibacterial suture, and a topical skin adhesive such as DERMABOND™ Mini Topical Skin Adhesive, or any appropriate dressing.
The patient is extubated, the Foley is removed, and the patient is taken to the recovery room.
Potential complications include but are not limited to:
Bleeding requiring reoperation
Note: If reoperation is necessary then an adjunctive hemostat such as SURGICEL SNoW™ or SURGICEL Powder™ might be a good option to control bleeding where primary methods (energy, staples, sutures, or clips) are ineffective or impractical.
- Surgical site infection (deep or superficial)
- Fecal fistula
- Conversion to open appendectomy
- Need for midline laparotomy
- Open wound
- Need for additional tests or procedures

Additional resources
Access our on-demand Colorectal video library
Looking for more? Explore procedural videos and webinars from global experts
Stapling Academy
This program offers interactive learning about the science of stapling and novel stapler design technologies.

Energy Academy
This program offers concise learning to understand monopolar, bipolar, and ultrasonic energy modalities.

