
George Crawford, MD
Laparoscopic Cholecystectomy
Procedure Overview
The gallbladder serves as a storage bin for bile, a digestive agent produced by the liver. Laparoscopic cholecystectomy is minimally invasive surgical removal of a gallbladder.
INDICATIONS & OBJECTIVES:
- Bilary Colic
- Cholelithiasis (gallstones in the gallbladder, commonly due to high cholesterol)
- Choledocholithiasis (gallstones in the common bile duct)
- Cholecystitis (inflammation of the gallbladder)
- Gallbladder Cancer
- Pancreatitis (Biliary)

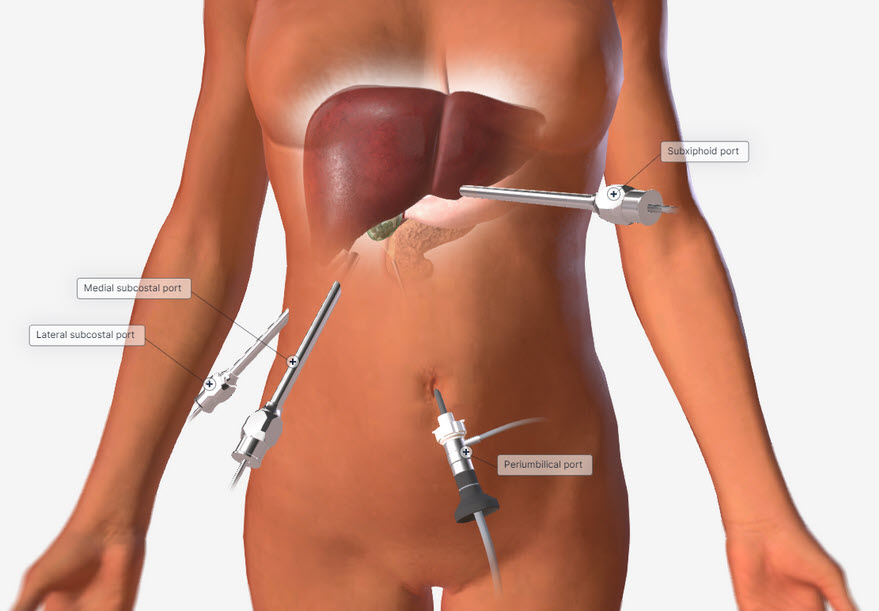
Common patient positioning:
- The patient is supine with the arms perpendicular to the body or tucked to the side.
The surgeon stands on the patient's left side, while the assistant stands on the patient's right.
Common port placement
- Periumbilical/camera port
- Lateral subcostal
- Medial subcostal
- Subxiphoid port
2. Repair
- The gallbladder is retracted superiorly and lateral.
- Electrocautery as well as blunt dissection is used to identify the Triangle of Calot.
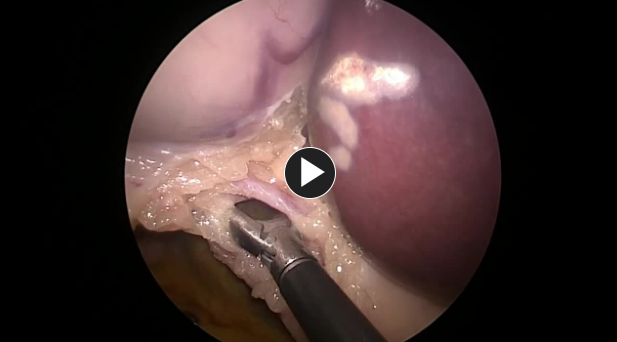
- The cystic duct is identified. Two clips are placed proximally, and one is placed distally.
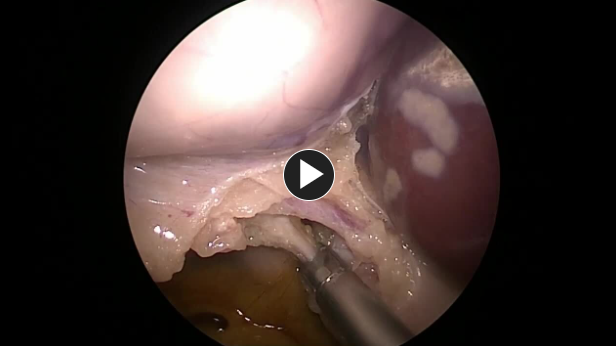
- The cystic artery is identified. Two clips are placed proximally, and one is placed distally.

- The cystic duct and the cystic artery are transected using scissors.
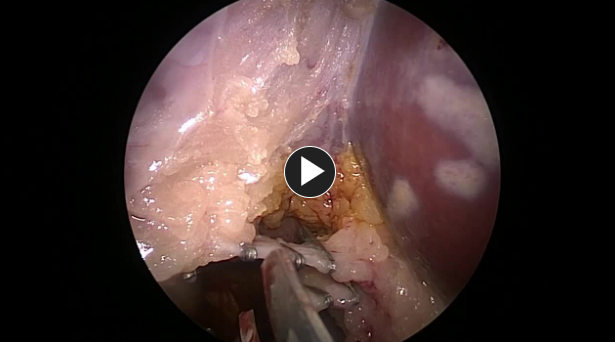
The gallbladder is removed from the gallbladder fossa using electrocautery or an ultrasonic energy device such as HARMONIC™ 1100.
Hemostasis is obtained while removing the gallbladder.
NOTE: Adjunctive hemostats such as SURGICEL SNoW™ or SURGICEL Powder™ may be used if the liver bed is oozing and where primary methods (energy, staples, sutures, or clips) are ineffective or impractical.

- The gallbladder is placed in an endoscopic specimen retrieval bag and removed through the 12 mm port.

3. Closure
- A suture like a size 0 Vicryl™ Plus Antibacterial suture, is used to reapproximate the fascia of the umbilicus.
- Commonly, a size 0 absorbable synthetic suture, like Vicryl™ Plus Antibacterial suture is used to close the fascia of the 12 mm trocar site.

- The remaining trocars are removed. The wounds are closed using synthetic absorbable suture, such as Monocryl™ Plus Antibacterial suture, and a topical skin adhesive such as DERMABOND™ MINI™ Topical Skin Adhesive, or any appropriate dressing.
The patient is extubated and taken to the recovery room.

Additional resources
Access our on-demand Upper GI & Abdominal video library
Looking for more? Explore procedural videos and webinars from global experts

Energy Academy
This program offers concise learning to understand monopolar, bipolar, and ultrasonic energy modalities.

