
Nezar Jrebi, MD
Laparoscopic Low Anterior Resection
Procedure Overview
Laparoscopic low anterior resection, involves removal of the sigmoid colon, upper, or mid and/or lower rectum affected by disease, followed by anastomoses to reconnect sigmoid/descending colon with the mid/lower rectum or anus.
INDICATIONS:
- Rectal Cancer
- Diverticular disease
- Inflammatory bowel disease
- GI bleeding
- Large polyp
- Rectal Prolapse

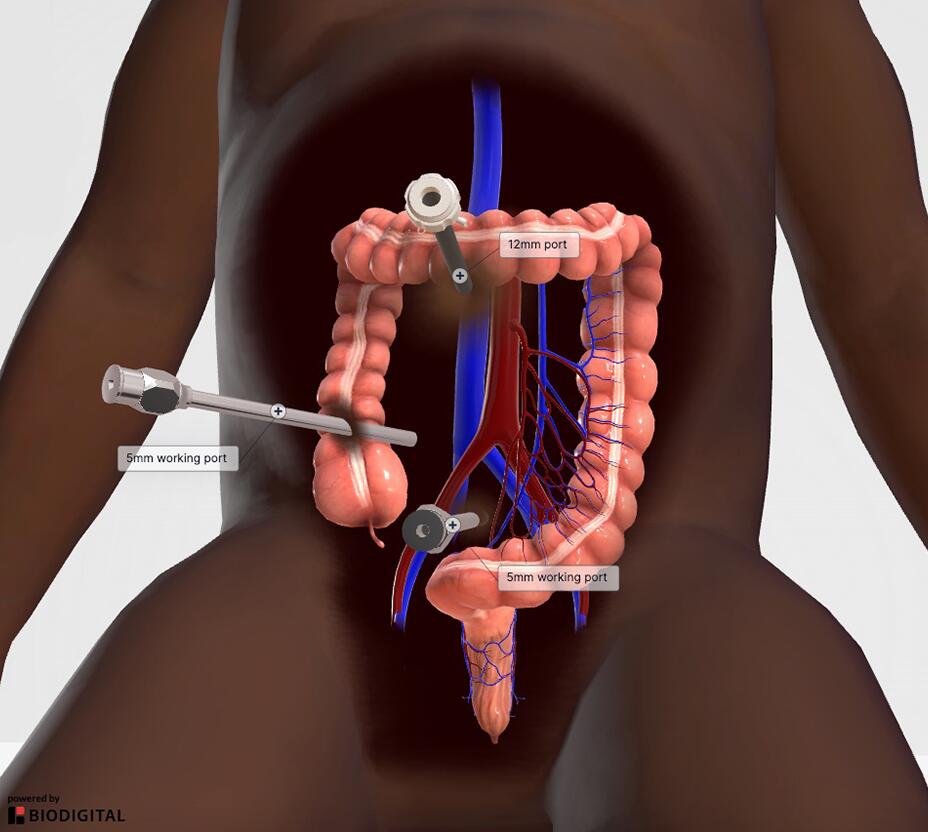
Common port placement
- Generally, 4 ports are used: three 5 mm and one 12 mm
- Must know tumor location prior to starting the case for proper trocar placement
- These factors/decisions will affect trocar placement
- Decide if vascular pedicles are stapled or energy is used
- Decide intracorporeal or extracorporeal anastomosis
- Colon extraction site
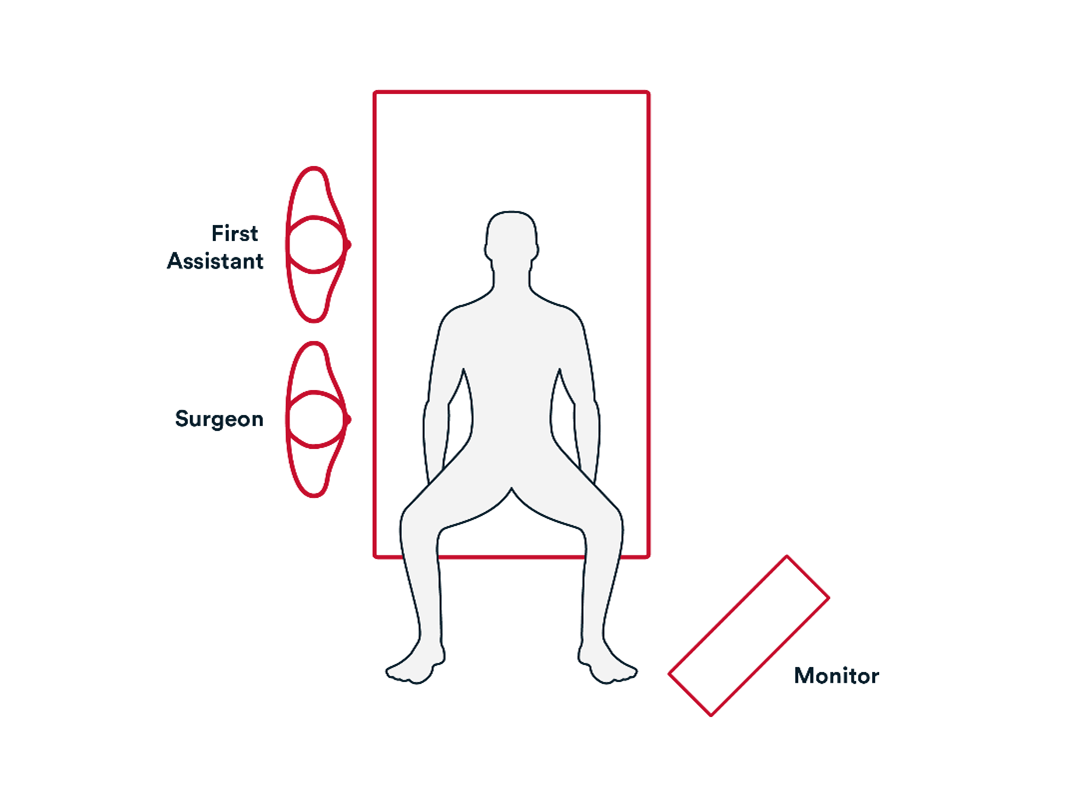
Common room setup
- Monitor is opposite from the surgeon
- Test all equipment before starting the procedure
- Heat and humidify CO2
- Intraoperative medications such as ICG, liposomal bupivicaine
- Recording device
Operative Steps
1. Access
- Initial Access to the abdomen is generally obtained by either:
- Veress needle technique.
- Direct trocar view technique.
- Trocar sites are identified, and trocars inserted to gain access to the abdominal cavity.

- Explore the abdominal cavity.
- Take down any adhesions.
2. Repair
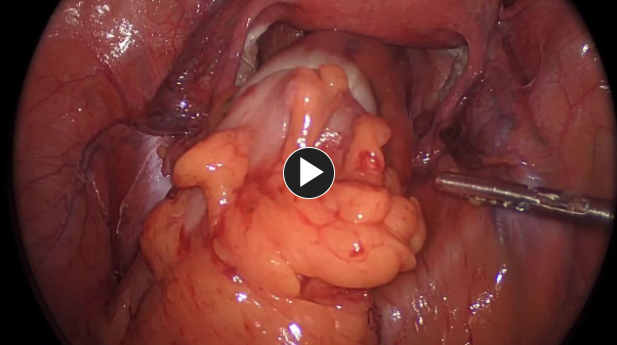
- Access and divide inferior mesenteric artery after identifying the left ureter.
- Gain access to and mobilize the cecum and ileum by ligating and dividing the ileocolic artery and ileocolic vein to their origins at the base of the mesentery, using an energy device such as ENSEAL™ X1 Curved Jaw Tissue Sealer or a stapling device such as ECHELON™ 3000 Stapler.
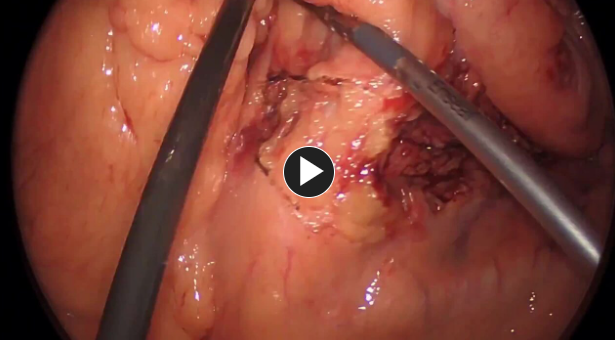
- Perform pelvic dissection.
- Transect rectum, using a stapling device, such as ECHELON™ 3000 Stapler.
- Mobilize the descending colon and splenic flexure with an energy device such as ENSEAL™ X1 Curved Jaw Tissue Sealer.
- Transect the proximal sigmoid colon using a stapling device, such as ECHELON™ 3000 Stapler and remove specimen.
- Perform end to end anastomosis, using a circular stapling device such as ECHELON™ Circular Powered Stapler.
- Consider diverting ileostomy in patients with preop radiation or very low anastomoses.
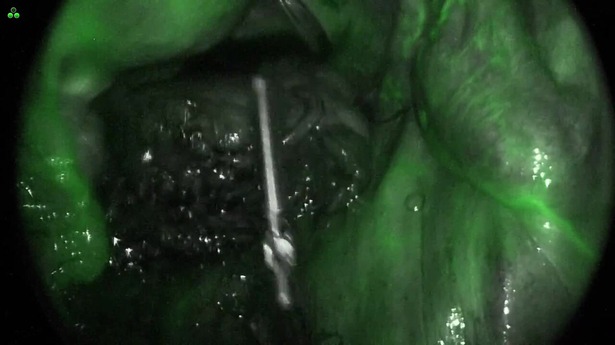
- Check the anastomosis for bleeding and leakage with a sigmoidoscope or colonoscope.
- May use ICG (indocyanine green).
- Remove fluid from wound and close the fascia using synthetic absorbable monofilament, such as PDS™ Plus Antibacterial suture.

- Subcuticular layer and skin are closed using synthetic absorbable monofilament, such as Monocryl™ Plus Antibacterial suture, and any appropriate dressing.
Potential complications include but are not limited to:
- Surgical bleeding
- Staple line Leak
- Wound infection
- Ileus
Additional resources

Access our on-demand Colorectal video library
Looking for more? Explore procedural videos and webinars from global experts
Stapling Academy
This program offers interactive learning about the science of stapling and novel stapler design technologies.

Energy Academy
This program offers concise learning to understand monopolar, bipolar, and ultrasonic energy modalities.

