
Nezar Jrebi, MD and Jay Redan, MD
Laparoscopic Right Hemicolectomy

Procedure Overview
Laparoscopic right hemicolectomy is one type of partial colectomy that involves removal of the terminal ileum to the mid-transverse colon. When performed for malignant disease an envelope of mesentery together with the corresponding lymphatic drainage with high ligation of supplying artery, this technique called Complete Mesocolic Excision (CME) followed by anastomoses to reestablish bowel continuity.
INDICATIONS:
- Colon cancer
- Unresectable polyps
- GI bleeding
- Inflammatory bowel disease
- Cecal Volvulus
- Diverticulitis
- Ischemic Colitis
- Intestinal Obstruction
- Appendiceal Tumor
- Neuroendocrine Tumor

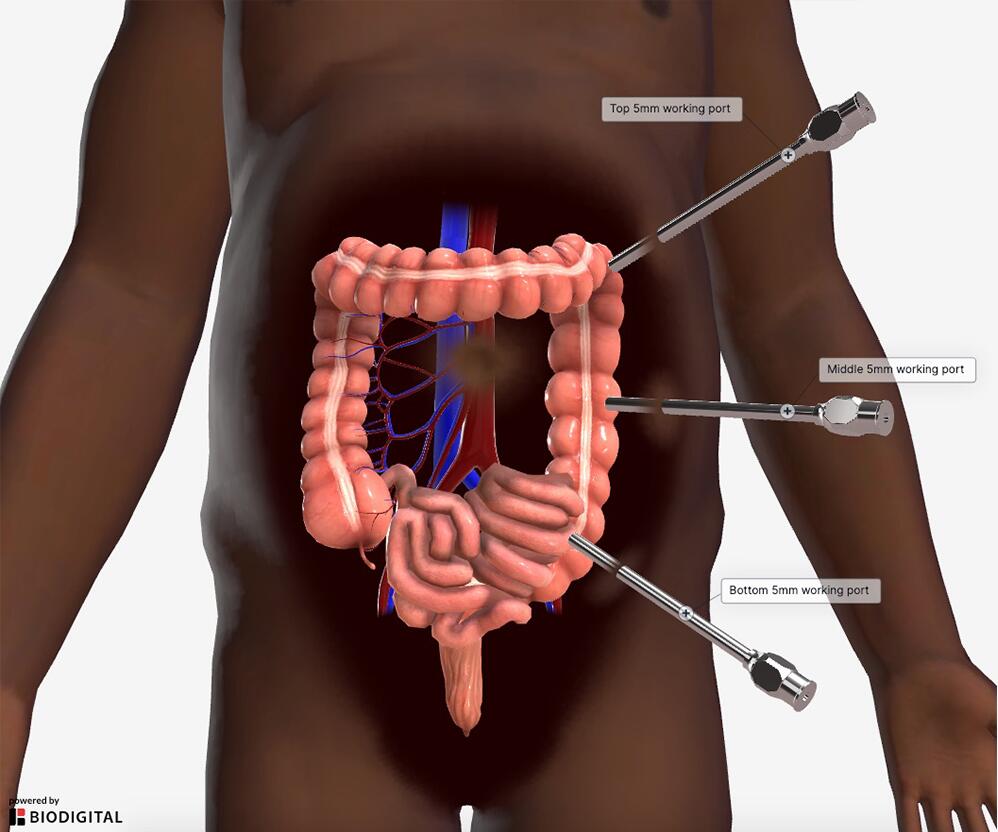
Common port placement
- Arrange ports thoughtfully in case conversion to hand assisted or open case will be required.
- Must know tumor location prior to starting the case for proper trocar placement.
- Generally, two to three 5 mm ports and one 12 mm port are used.
- These factors/decisions will affect trocar placement.
- Decide if vascular pedicles are stapled or energy is used.
- Decide intracorporeal or extracorporeal anastomosis.
- Colon extraction site.
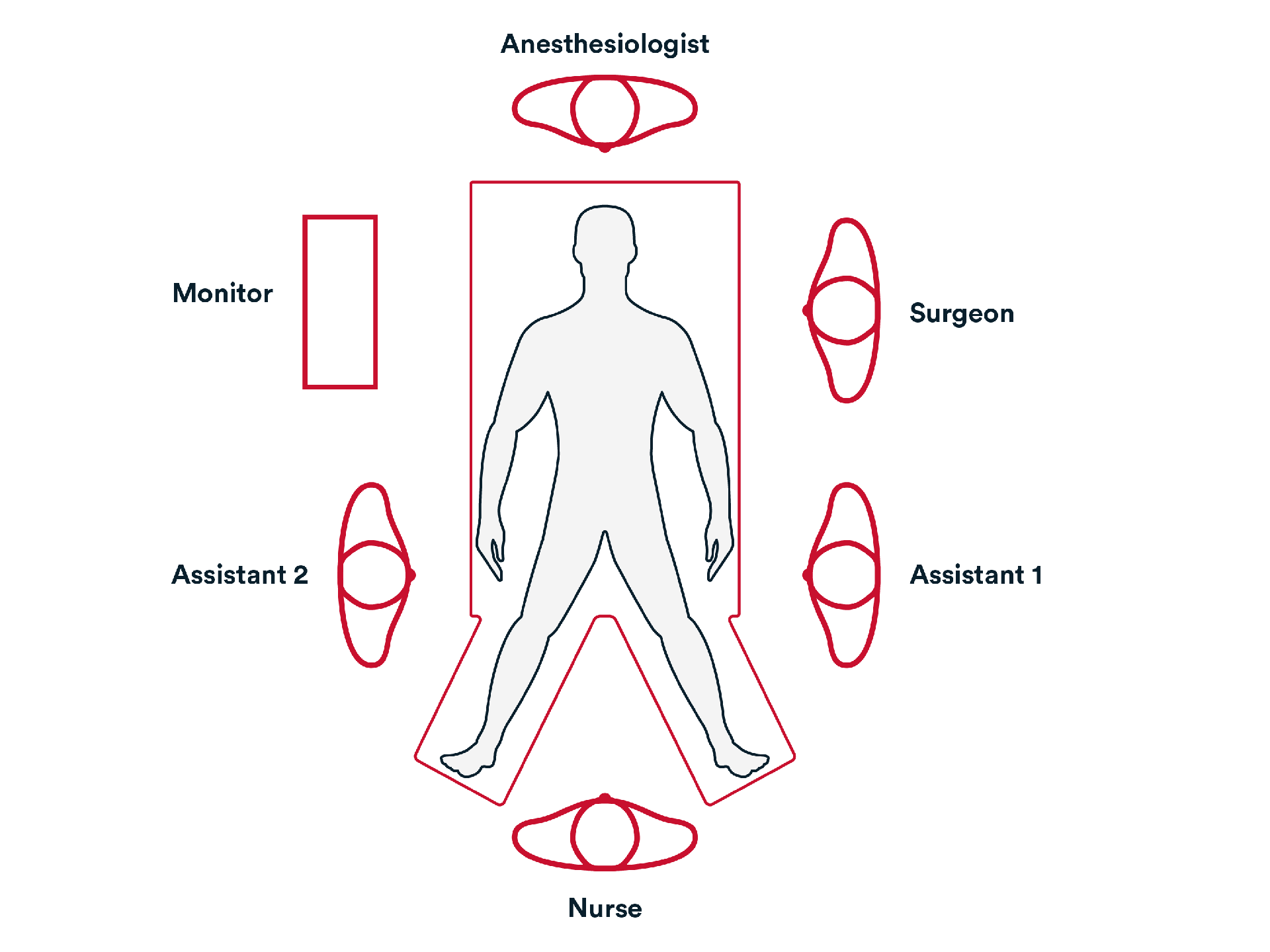
Common room setup
- The surgeon is usually on the patient’s left side with the assistant.
- Monitor is opposite from the surgeon.
- Recording device is available.
Operative Steps
1. Access
- Initial Access to the abdomen is generally obtained by either:
- Veress needle technique.
- Direct trocar view technique.

- Trocar sites are identified, and trocars inserted to gain access to the abdominal cavity.

- Gain access to and mobilize the cecum and ileum by ligating and dividing the ileocolic artery and ileocolic vein to their origins at the base of the mesentery, using an energy device such as ENSEAL™ X1 Curved Jaw Tissue Sealer or a stapling device such as ECHELON™ 3000 Stapler.
- Continue mobilization and dissect the hepatic flexure and right transverse colon mesentery by ligating and dividing the right middle colic vessels using an energy device such as ENSEAL™ X1 Curved Jaw Tissue Sealer.
- Ensure a complete specimen with intact mesocolic envelope containing all lymph nodes, extract specimen.
- Perform a side to side or end to side anastomosis, using a stapling device such as PROXIMATE™ Linear Cutters.
- Check the anastomosis for bleeding and leakage.
- Close the common enterotomy using a stapling device or suture such as Monocryl™ Plus Antibacterial suture or STRATAFIX™ Spiral MONOCRYL™ Plus Knotless Tissue Control Device and reinforce the staple line intervention if applicable.
- Remove fluid from wound and close the fascia using suturing device such as STRATAFIX™ Symmetric PDS™ Plus Knotless Tissue Control Device.
Additional resources

Access our on-demand GYN video library
Looking for more? Explore procedural videos and webinars from global experts

Energy Academy
This program offers concise learning to understand monopolar, bipolar, and ultrasonic energy modalities.

