
Young K. Hong, MD
Right Hepatectomy
Procedure Overview
Right hepatectomy is a formal anatomic resection of right lobe of liver. The inflow and outflow of the liver blood supply is controlled prior to parenchymal transection. Here we outline the steps for right hepatectomy.
INDICATIONS & OBJECTIVES:
- Primary hepatocellular carcinoma
- Colorectal liver metastasis
- Metastatic neuroendocrine tumor
- Primary intrahepatic cholangiocarcinoma
- Hilar cholangiocarcinoma
- Symptomatic giant hemangioma

Prep & Patient Positioning
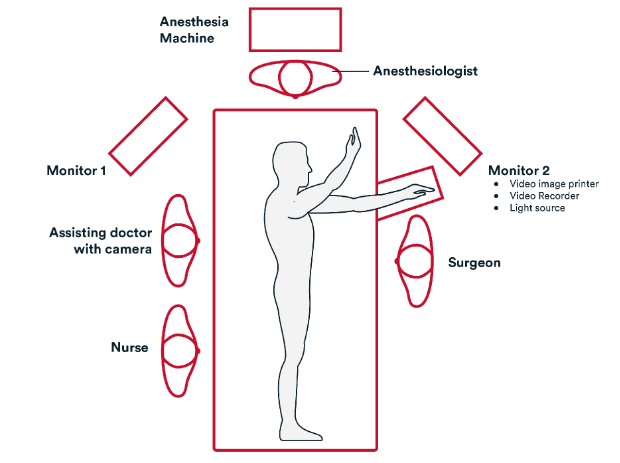
Common room setup
Common patient positioning:
- Typically, the patient is placed in the supine, depending on surgeon preference
- Arms out to allow access for anesthesia for additional lines
Surgeon can be on either side of the patient - Assistant is opposite from surgeon
- IMPORTANT: Patient secured to the table
- OG (oral-gastric) tube
- Venous compression boots
- Foley catheter
Operative Steps
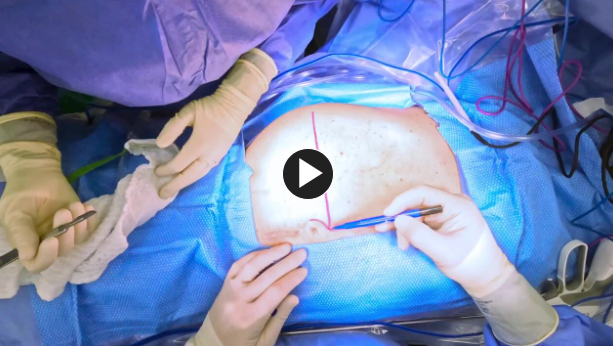
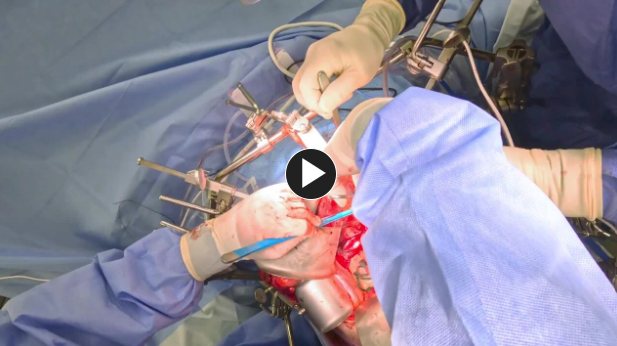
1. Access
Incision:
- Modified Makuuchi incision is utilized to maximize visibility while lower pain compared to subcostal incision, especially after TAP block (anesthetic/nerve block) along the lateral incision.
- Thompson bar or a similar retractor on patient’s right side should have lower bar lowered as much as possible to allow in-line view of vena cava during mobilization portion.
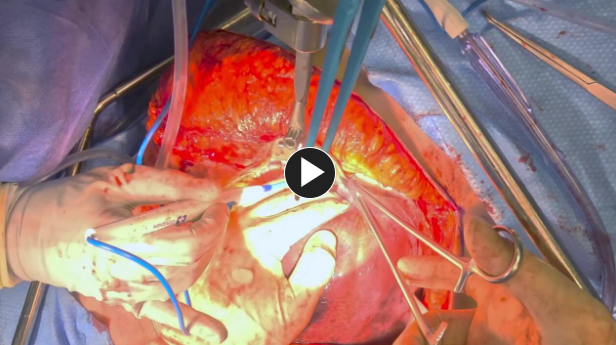
Mobilize Liver:
- Take down the falciform ligament and bilateral coronary/triangular ligaments for optimal mobilization to minimize stress on left liver when retracting the liver.
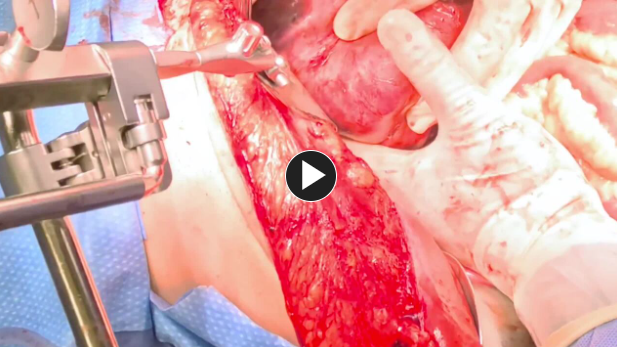
Retrohepatic vena cava mobilization should take caution to ligate small short retrohepatic vein attachments.
- Retrohepatic suspensory ligament or Makuuchi ligament is transected to visualize right hepatic vein insertion in order to encircle the vessel.
Inflow Control:
- Dissect portal hilum to isolate the right hepatic artery and right portal vein.
- Be sure to test clamp and confirm blood flow to left liver prior transection
Outflow Control:
- Right hepatic vein is encircled and transected with vascular stapler, such as ECHELON FLEX™ Powered Vascular Stapler.
- Important to transect the Makuuchi ligament to visualize the insertion of right hepatic vein
2. Repair
Parenchymal Transection:
- Using an energy device, transect along the line of demarcation of ischemic liver.
- Pringle maneuver is utilized during transection – important to have operative team track time on pringle maneuver and allow adequate time to re-pringle.
- A combination of bipolar, ultrasonic and mechanical methods utilizing devices such as ENSEAL™ X1 Curved Jaw Tissue Sealer, are used for dissection to transect the liver.
- Important to coordinate with anesthesia to minimize fluid resuscitation to prevent retrograde flow within liver and minimize hemorrhage.
- Frequent use of ultrasound throughout case is critical and must be familiar with ultrasound technique.
3. Closure
- Resuspend the falciform ligament to minimize complication of liver torsion after hepatectomy.
- Place figure of eight synthetic absorbable suture such as #0 Vicryl™ Plus Antibacterial Suture to approximate the umbilicus prior closing the lateral incision.
- Fascia is closed in a running fashion using a synthetic absorbable suture such as #1 PDS™ Plus Antibacterial Suture.
- Skin closure is performed using a synthetic absorbable suture such as such as Monocryl™ Plus Antibacterial sutures and a topical skin adhesive such as Dermabond™ Prineo Skin Closure System.
Post-operative Patient Care
Typical recommendations for post-operative care may include, but are not limited to, any of the following:
- Remove foley catheter early if placed intraoperatively.
- ERAS protocol includes use of non-narcotic pain control with acetaminophen, gabapentin, and celecoxib as well as early and frequent ambulation and aggressive pulmonary toilet.
(Back to the top)
Additional resources
Access our on-demand Bariatric video library
Looking for more? Explore procedural videos and webinars from global experts
Stapling Academy
This program offers interactive learning about the science of stapling and novel stapler design technologies.

Energy Academy
This program offers concise learning to understand monopolar, bipolar, and ultrasonic energy modalities.

