
Keith D. Mortman, MD
Thoracoscopic Lobectomy
Procedure Overview
Thoracoscopic lobectomy is a minimally-invasive, anatomic resection of one of the lobes of the lung. It involves the division of the arterial supply, venous drainage, and airway to the lobe. It is typically (although not exclusively) performed for lung cancer.
INDICATIONS:
- Primary lung cancer
- Solitary metastatic cancer to the lung
- Pulmonary sequestration
- Arteriovenous malformation

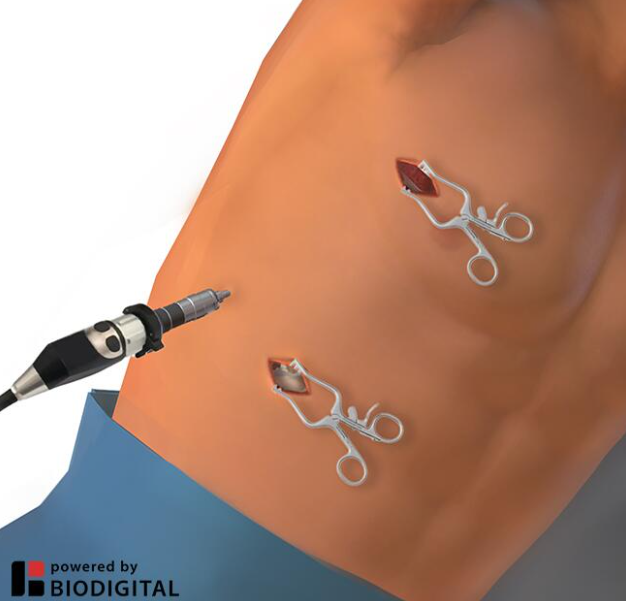
Common port placement
- Traditional disposable ports not required. One 5mm reusable metal port used for the scope.
- A 2cm paracostal incision is made in the interspace above the diaphragm and below the breast.
- A 5mm incision is made in the midaxillary line at the 8th intercostal space (ICS).
- All lobectomies start with these 2 incisions.
- A 4cm accessory incision is made in the anterior axillary line at the 4th ICS (for upper lobectomies) or 5th ICS (for middle or lower lobectomies).
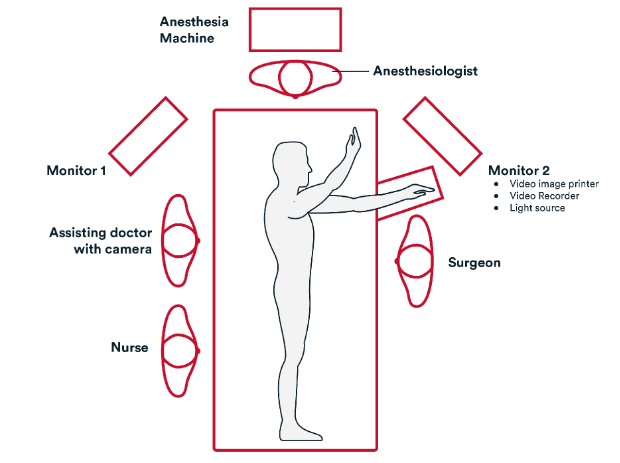
Common room setup
- The surgeon is positioned towards the patient’s front with the assistant towards the patient’s back.
- 2 monitors are placed near the head of the bed at 45-degree angles to the surgical table.
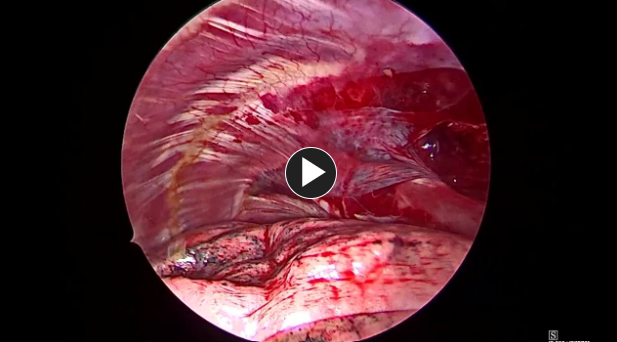
- Perform manual palpation of the entire lung to rule out occult disease and to ensure resectability of primary lesion.
- If not yet performed, completely mobilize the inferior pulmonary ligament.
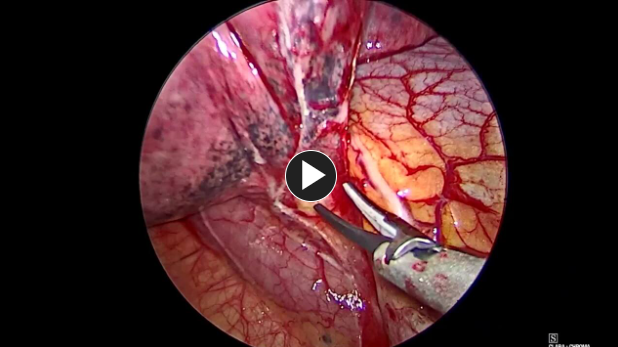
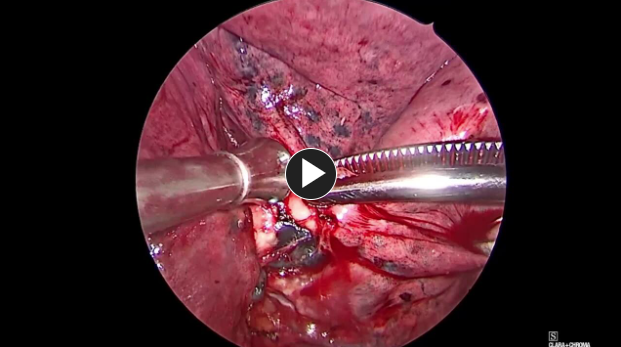
- Retract the lung anteriorly and complete a posterior lymphadenectomy including stations 7, 8, and 10 with the Harmonic 1100 Shears.
- Retract the lung posteriorly and complete the anterior hilar dissection removing level 10 and 4R inferior (on the right side) with the Harmonic 1100 Shears.
DISSECTING & DIVIDING BLOOD VESSELS
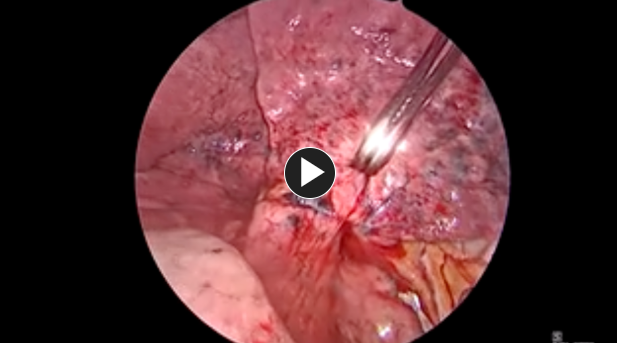
- For upper and middle lobes, dissect the upper and middle lobe pulmonary vein as it lies more anterior to the artery.
- For lower lobectomies, the inferior pulmonary vein is found at the base of the inferior pulmonary ligament.
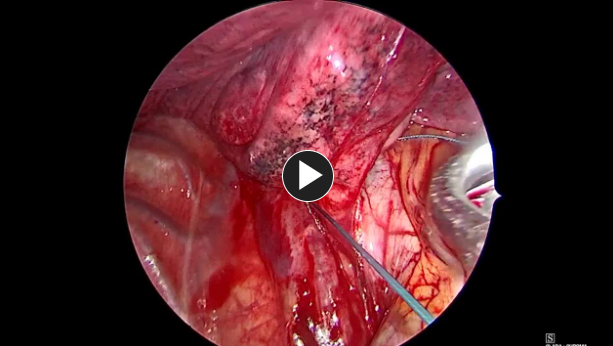
- Encircle the vein with a suture or vessel loop to aid in manipulation for stapling.
- Remove level 11 and 12 lymph nodes with the Harmonic 1100 Shears.
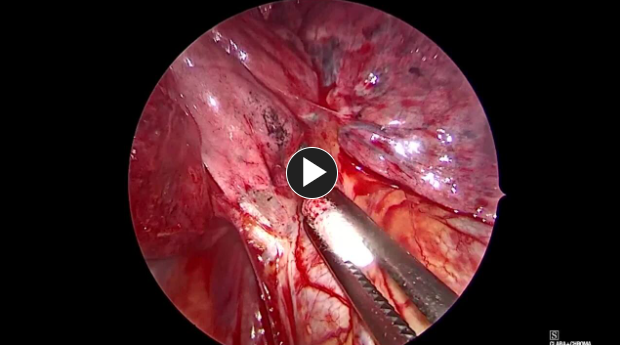
- Dissect out the lobar branches of the pulmonary artery and encircle with a suture or vessel loop.
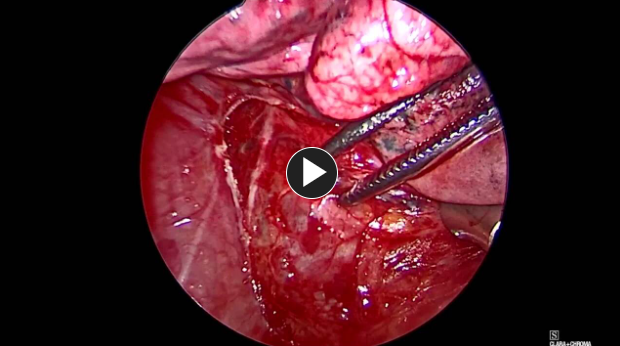
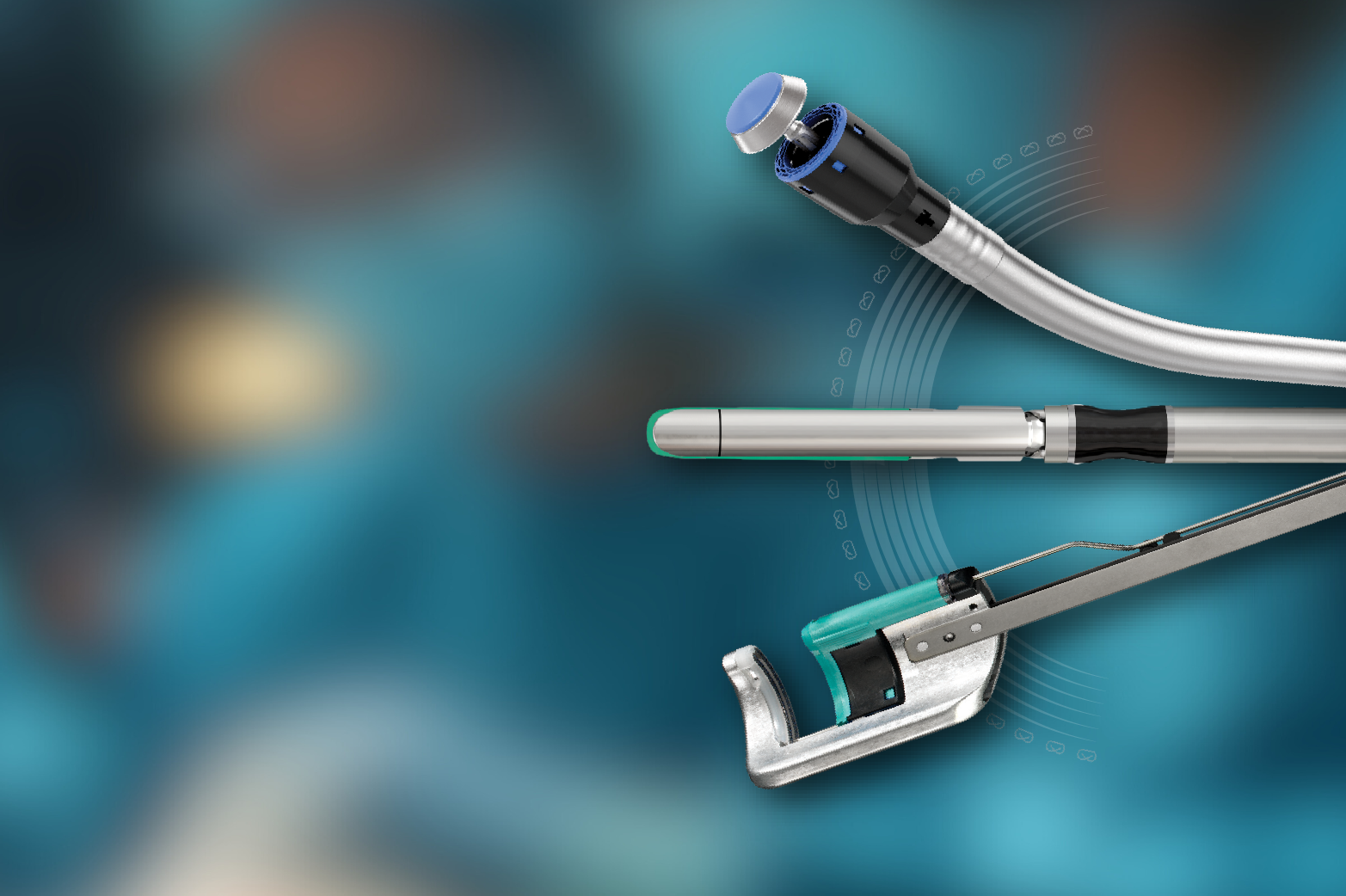
- Staple and divide the pulmonary artery to the lobe using the ECHELON FLEX™ PVS.
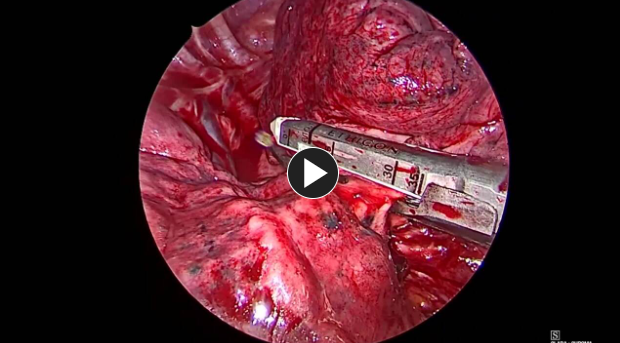
- Using the ECHELON FLEX Powered Vascular Stapler (PVS), staple & divide the pulmonary vein.
- Dissect and encircle the lobar bronchus with a suture or vessel loop.
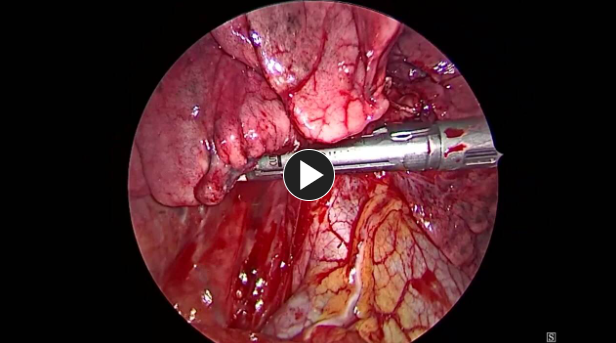
- Compress the lobar bronchus with the ECHELON 3000 stapler (Green load).
- Perform test ventilation to ensure no inflation of target lobe with adequate ventilation to remaining lung.
- Staple and divide lobar bronchus with the ECHELON 3000 stapler (Green load).
- Remove the specimen from the chest in an appropriately sized tissue pouch.
- Complete the lymphadenectomy by removing level 2R and 4R on the right side, or level 5 and 6 on the left side with the Harmonic 1100 Shears.
AIR LEAK TEST
- With all staple lines and lung parenchyma under saline, gradually ventilate the lung. Start at an airway pressure of 20cmH2O and increase in increments of 5cmH20 up to 35cmH20 while examining the lung for evidence of an air leak.
4. Closure
- Suction any remaining irrigation fluid.
- Place a single chest tube to the apex of the chest and secure.
- The deep and superficial subcutaneous tissue is closed with #2-0 Vicryl™ Plus Antibacterial sutures.
- Skin is closed with #4-0 PDS™ Plus Antibacterial sutures or Monocryl™ Plus Antibacterial sutures.
NOTE: “Debrief” with the O.R. team should verify the procedure performed, estimated blood loss, correct labeling of all pathology specimens, and anticipated postoperative needs.
Potential complications include but are not limited to:
- Air leak
- Bleeding
- Atelectasis
- Pneumonia
- Arrythmia
- Wound infection
Post-operative Patient Care
Typical recommendations for post-operative care may include, but are not limited to, any of the following:
- Remove foley catheter early if placed intraoperatively.
- ERAS protocol includes use of non-narcotic pain control with acetaminophen, gabapentin, and celecoxib as well as early and frequent ambulation and aggressive pulmonary toilet.
(Back to the top)
Additional resources
Access our on-demand Bariatric video library
Looking for more? Explore procedural videos and webinars from global experts
Stapling Academy
This program offers interactive learning about the science of stapling and novel stapler design technologies.

Energy Academy
This program offers concise learning to understand monopolar, bipolar, and ultrasonic energy modalities.

