
Grace Chen, MD
Total Abdominal Hysterectomy
Procedure Overview
Hysterectomy options exist for benign diseases with the route of hysterectomy influenced by several factors. A variety of surgical approaches exist for the removal of the uterus, including vaginal, abdominal, or minimally invasive. The size and shape of the uterus, and the indication for removal determine the most optimal approach for the patient. An abdominal hysterectomy is an operation to remove the uterus and cervix with or without the ovaries and fallopian tubes via the abdominal route. This abdominal laparotomy approach requires opening the abdominal wall for tissue removal.
INDICATIONS:
Abdominal hysterectomy may be done for different reasons, including, but not limited to:
- Uterine fibroids that cause bothersome pressure, bleeding, or other problems
- Abnormal uterine bleeding
- Ovarian and Tubal disease
- Endometriosis
- Pelvic adhesive disease

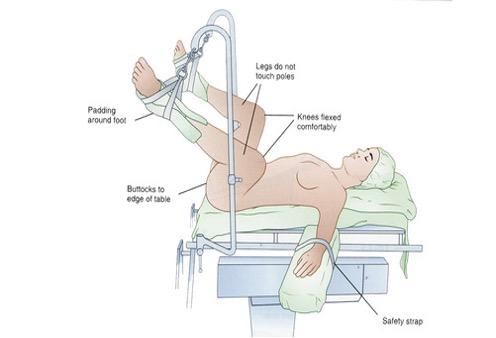
Common Patient Positioning
- The patient is placed in the dorsal lithotomy position in Allen Stirrups or in the supine position and her arms outstretched on arm boards or tucked at her sides.
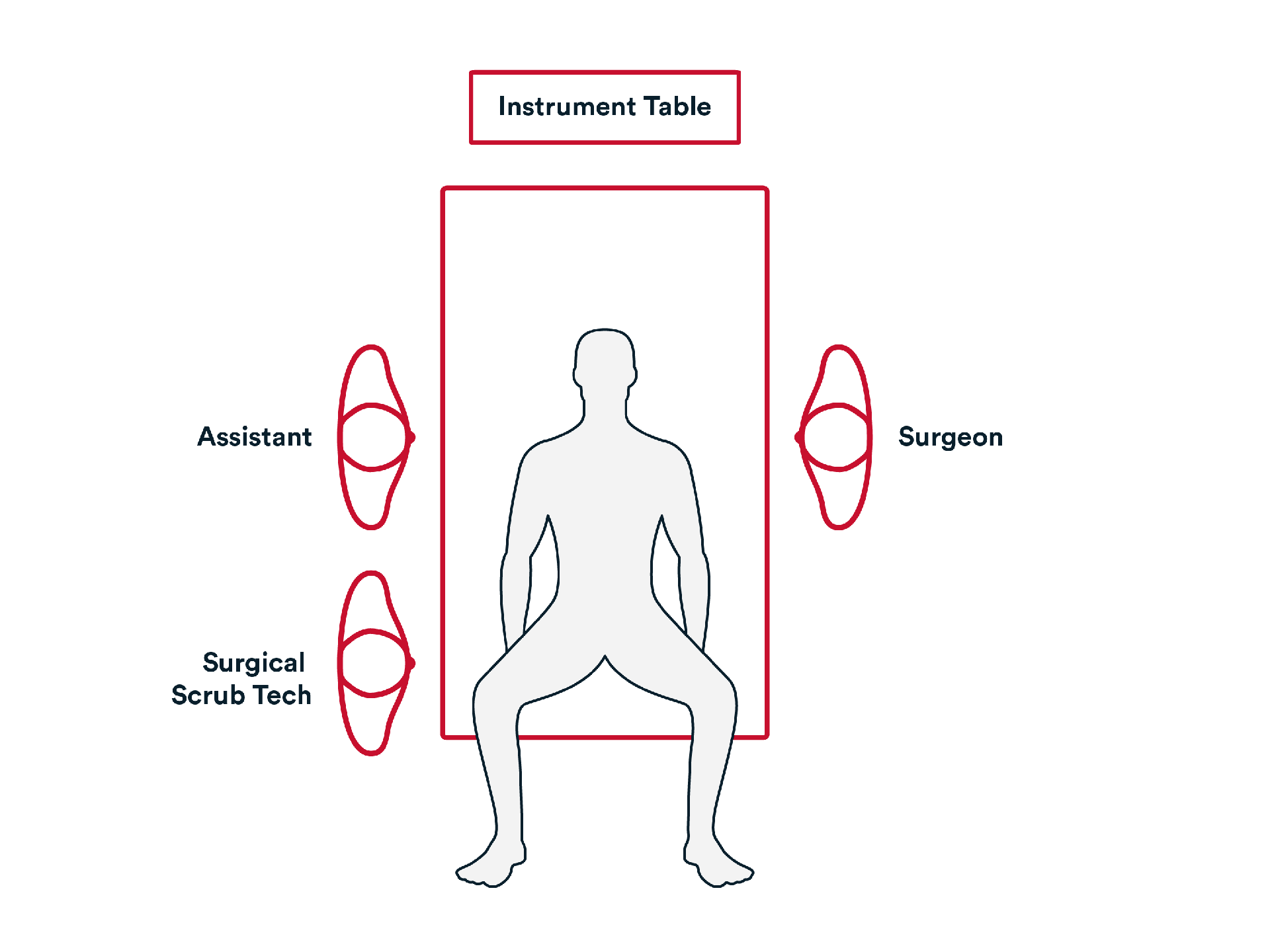
Common room setup
- The patient is prepped and draped in the usual fashion for an abdominal procedure.
- The primary surgeon is usually standing on the left side of the patient with one assistant on the right side of the patient beside the surgical scrub technician.
- The abdominal hysterectomy tray is open on the back table, suction irrigation is hooked up and surgical energy is available.
2. Repair
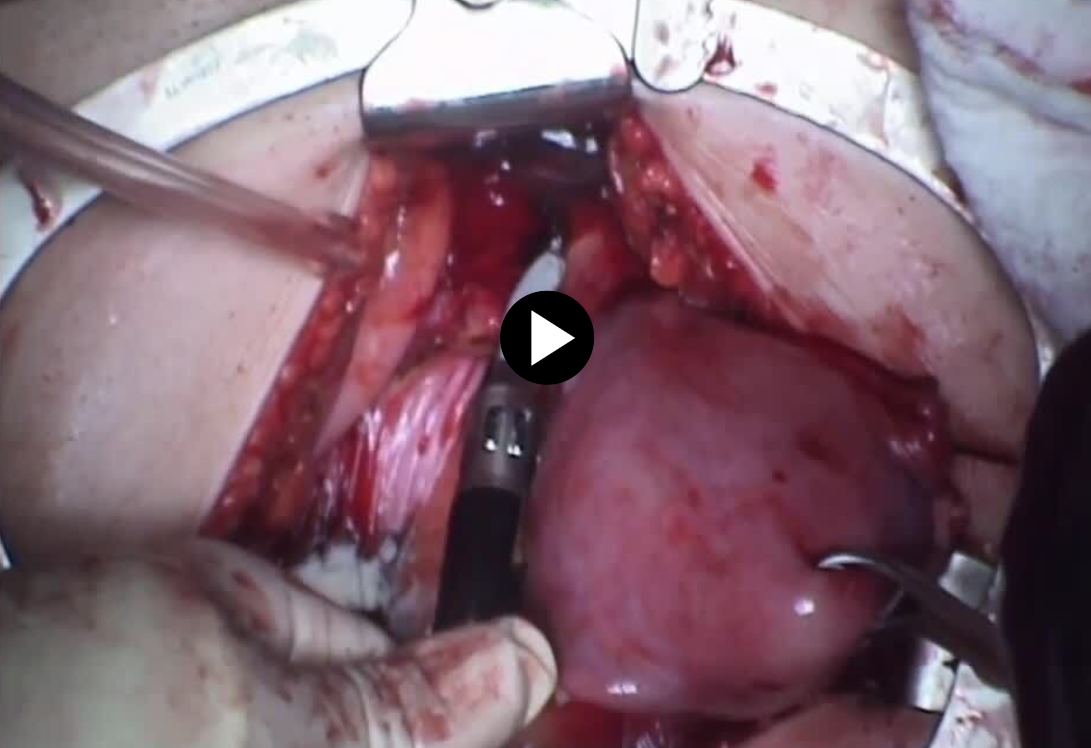
- The mesosalpinx (if the ovary is retained) or infundibulopelvic ligament (if the ovary is being removed) is clamped coagulated and cut.
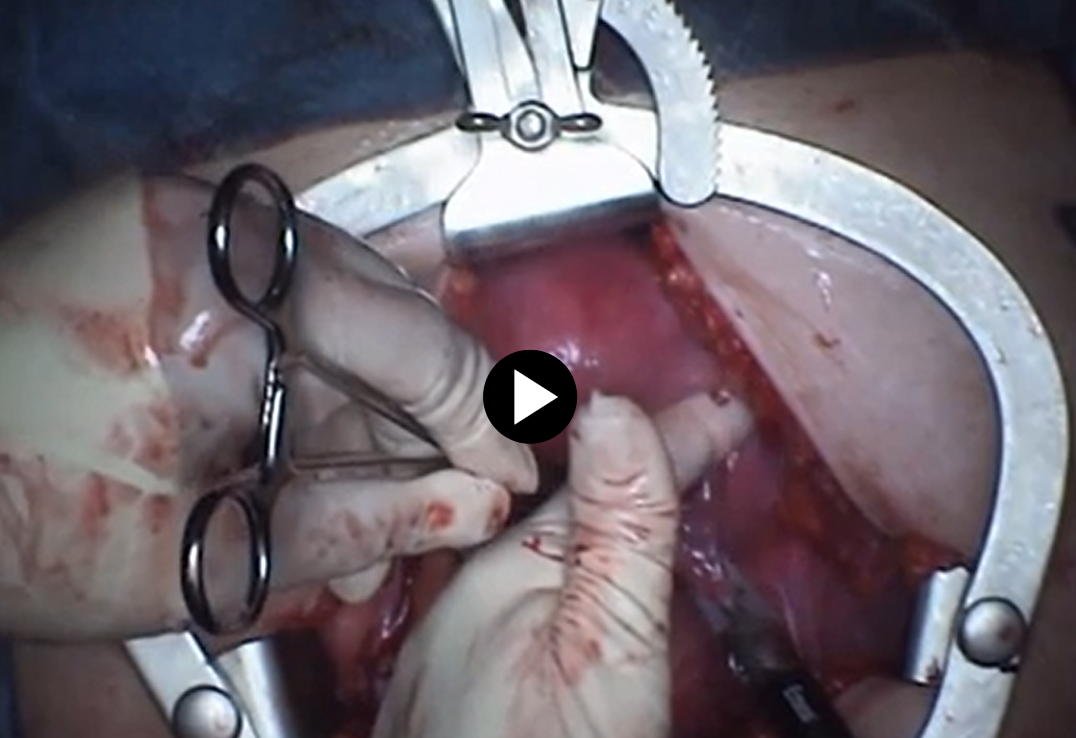
- With successive clamping, coagulating, and cutting, the dissection continues down the broad ligament to the uterine vessels.

- The anterior bladder peritoneum is incised with scissors and the bladder is pushed down with the sponge stick forceps. Broad ligament is pushed forward with the surgeons’ fingers.
- Using Enseal X1 Large Jaw the Uterine vessels are divided. 0-Vircyl plus suture with CT-1 needle to cut out the vessels can be used.
- Placing right angle hysterectomy clamps, the cervical vaginal junction is incised and the uterus and cervix are removed.
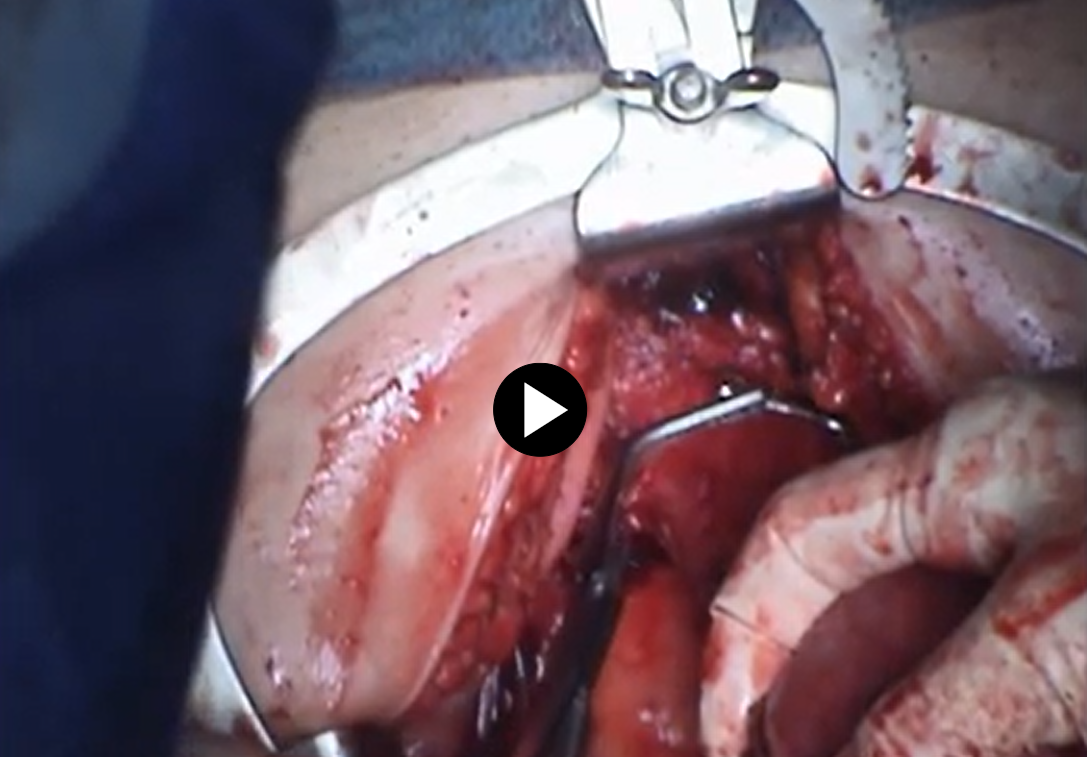
- Grasping the anterior vaginal mucosa place your first bite with a barbed suture such as 2-0 Stratifix Knotless Tissue Control Device.
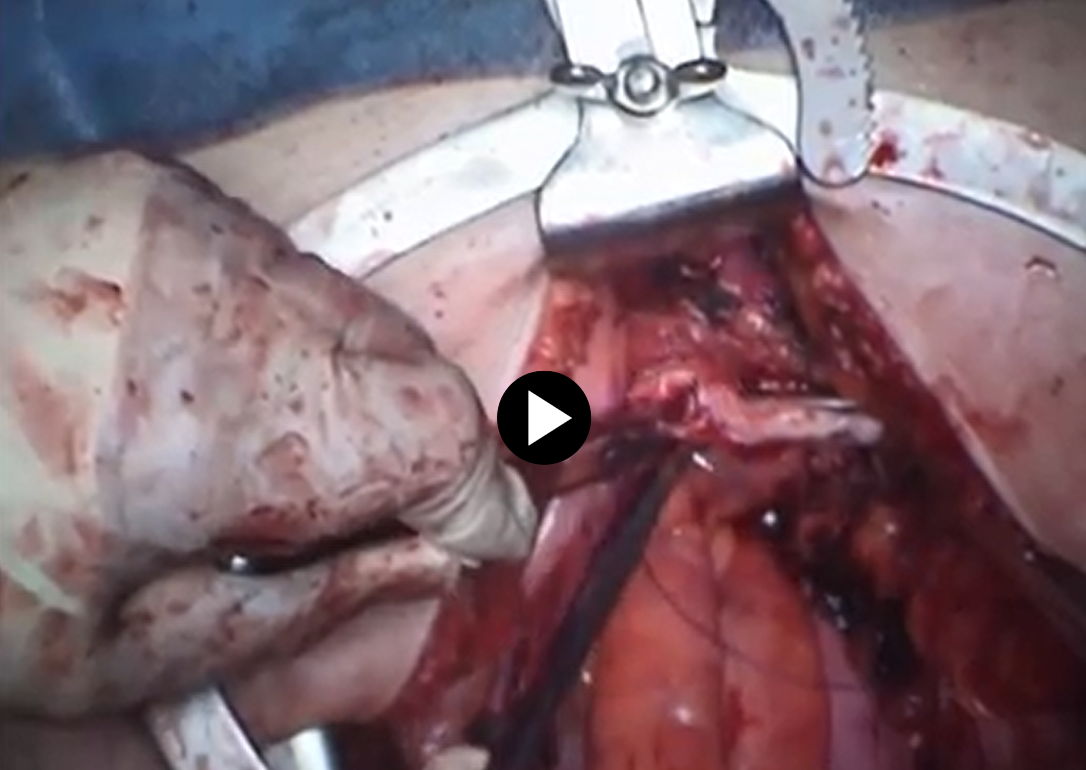
- Place Suture on the uterosacral ligament incorporate this as your second closure bite.
- Suture the posterior angle to complete the angle closure (Only the angles have three bites for closure).
- Run the suture anteriorly to posteriorly, making sure full-thickness bites are taken, to the opposite angle.
- Lastly, complete the angle in a similar manner as previously mentioned (3 bites).
Back track the suture one or two bites then cut the remaining suture.
Note: Vaginal cuff can be closed using 0-Vicryl Plus suture in a continuous or interrupted technique.
4. Abdominal Wall Closure
- 2 x size 0 Stratafix Symmetric Knotless Tissue Control Device is used to approximate the fascial layer.
(Back to the top)

Post-operative Patient Care
Typical recommendations for post-operative care may include, but are not limited to, any of the following:
- Patients should improve each day postoperatively, temperature greater than 100.4, and increasing abdominal pelvic pain not relieved by
- Typical discharge instructions consist of medications for pain management and bowel regularity, diet, and activities, clinic follow-up in 2 weeks.
- Most patients will be discharged the same day or 23 hours stay.
Patients are recommended to follow any nutritious diet that they can tolerate and generally first try liquids and foods that may be easily digestible. - Patients are encouraged to ambulate early (with assistance if needed) even on the day of surgery to reduce deep vein thrombosis (DVT) risk.
- Generally, patients are asked to be active as they can tolerate but limit strenuous activities.
Additional resources

Access our on-demand GYN video library
Looking for more? Explore procedural videos and webinars from global experts

GYN Registrar Program
GYN specialty based tailored learning curriculum demonstrating technique and best practice in lap skills and suturing

Energy Academy
This program offers concise learning to understand monopolar, bipolar, and ultrasonic energy modalities.
SuturED
This program offers interactive learning about the science of stapling and novel stapler design technologies.

