
Steven McCarus, MD
Laparoscopic Myomectomy

Procedure Overview
Removal of fibroids from the uterus, the most common location of fibroids, is termed myomectomy. Myomectomy is the technique most used for symptomatic uterine fibroids in patients who are desirous of future fertility or uterine preservation. The minimally invasive approach is preferred over abdominal when feasible and appropriate. The selection may be influenced by the number of fibroids that need to be removed and the surgeons experience.
INDICATIONS & OBJECTIVES:
A hysterectomy is an operation to remove the uterus. This surgery may be done for different reasons, including, but not limited to:
- Removal of uterine fibroids may be done for different reasons, including, but not limited to:
- Prolonged menstrual bleeding
- Heavy menstrual bleeding
- Pelvic pressure and urinary frequency
- Abdominal bloating
- Rectal Pressure
- Dyspareunia

Relevant Anatomy
Click to interact with a BioDigital Human animated 3D anatomy, disease states, and procedure tour.
Pre-operative Patient Care
Typical recommendations for pre-operative care may include, but are not limited to, any of the following:
- The meal the night before should be light and easily digestible.
- Nothing by mouth from midnight the day before surgery.
- Routine labs, HCG, CBC, UA, Type and Screen with prophylactic broad-spectrum antibiotics as well as ERAS medication ordered and/or given.
- Any other comorbidities may require other preoperative tests or medical clearance.
- All preoperative imaging of the pelvis (MRI, ultrasonography and computed tomography) should be available for review as needed. Informed consent obtained by the operating surgeon must be completed and witnessed.
Prep & Patient Positioning
Common patient positioning:
- Patient is placed in the dorsal lithotomy position in Allen stirrups with buttock at
- The knee, ankle and hip joints are in plane with feet down.
- The patients' arms are tucked at the bedside and secured.
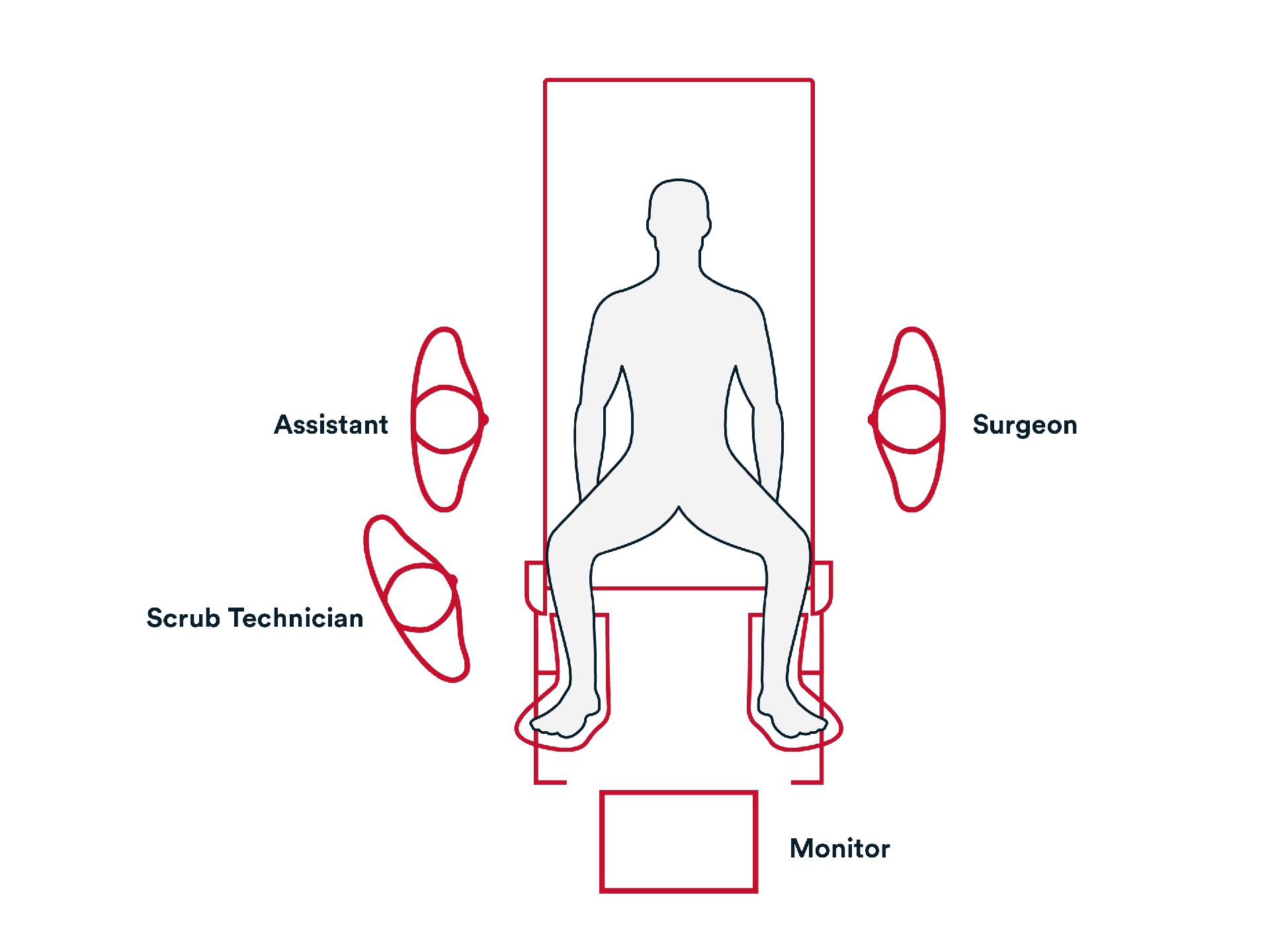
Common room setup:
- The patient is prepped and draped in the usual fashion for a laparoscopic procedure.
- The primary surgeon is usually standing at the patient’s left with the assisting surgeon and one scrub assistant on the patient’s right side.
- The mayo tray at the patient’s feet with laparoscopic instruments available and the back table with other needed items.
- The monitor is positioned at the foot of the bed.
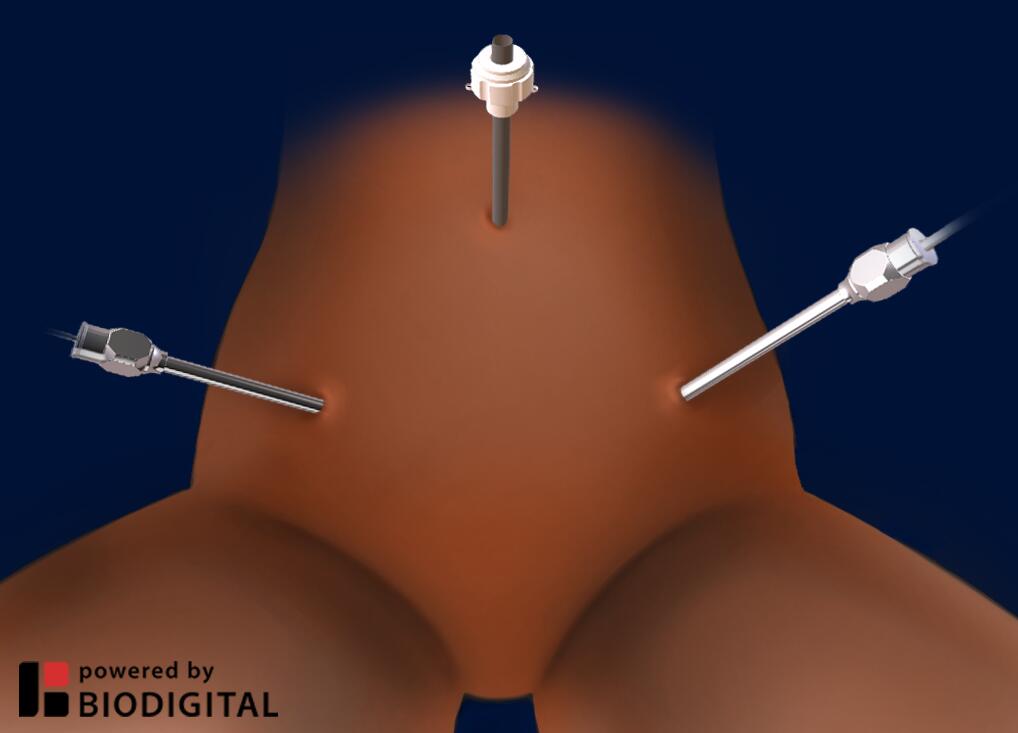
Common port placement:
- 5 mm trocar at the umbilicus
- 11 mm trocar at the Left lower quadrant
- 11 mm trocar at the Right lower quadrant
Operative Steps

Access
Access
- The abdominal wall is elevated, an Ultra Veress Needle is placed through the umbilicus, CO2 gas is insufflated.
- A small skin incision is made at the umbilicus, then a non-bladed 5 mm trocar such as ENDOPATH XCEL™ Trocar is passed through the incision, confirmation that you are in the abdominal cavity is made with the laparoscope.
- Once the patient is in the Trendelenburg position, a 2nd and 3rd 11mm non-bladed trocars are passed through the abdominal wall.
Repair
Repair
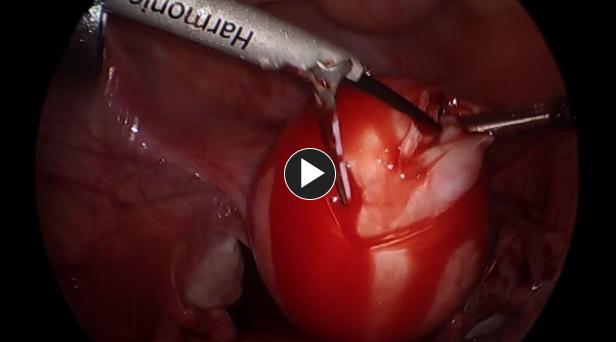
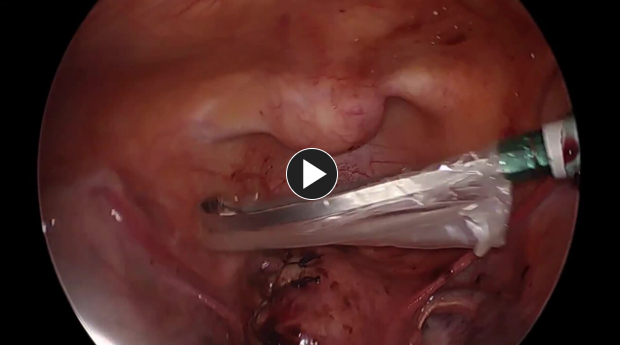
- Once the location of the fibroid is identified, Vasopressin is injected until blanching of the tissue is noticed.
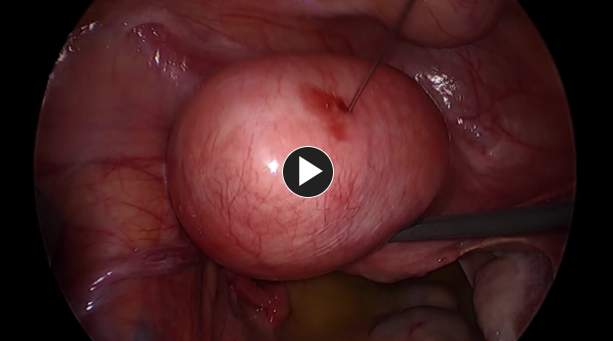
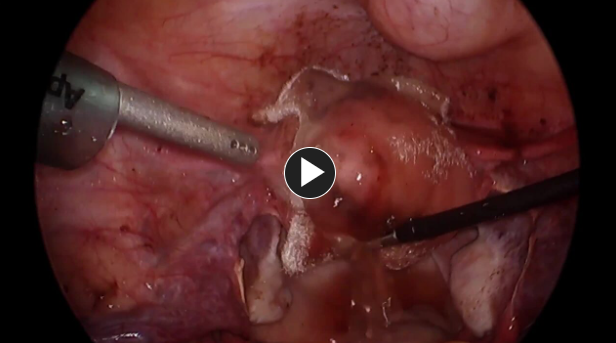
- Securing the uterus with a grasper, HARMONIC™ 1100 is then used to cut the serosa covering the fibroid. This will expose the fibroid. Using traction and countertraction, the fibroid will be disengaged from the uterus.
- Myoma vessel control is accomplished by using an energy device such as HARMONIC™ 1100 as needed.
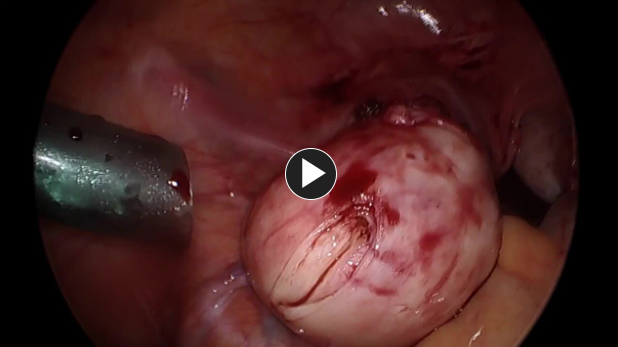
- Use Topical absorbable hemostatic agent such as SURGICEL™ Powder Absorbable Hemostat on the fibroid site for hemostasis as necessary.
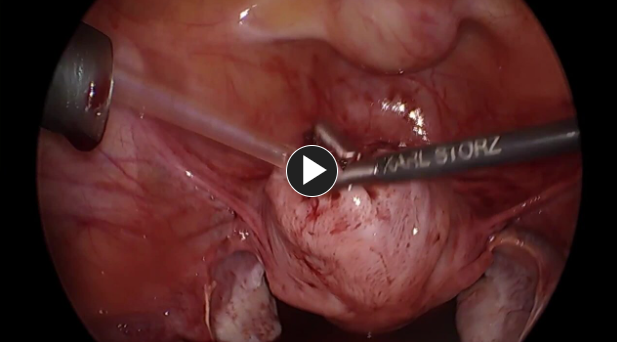
- Closure of the defect with a synthetic absorbable suture such as size 0 Vicryl-Plus suture, with CT-1 needle.
- If needed, the deep myometrium can be closed with a knotless tissue control device such as STRATAFIX™ Knotless Tissue Control Device, then followed by synthetic absorbable suture such as Vicryl-Plus suture.
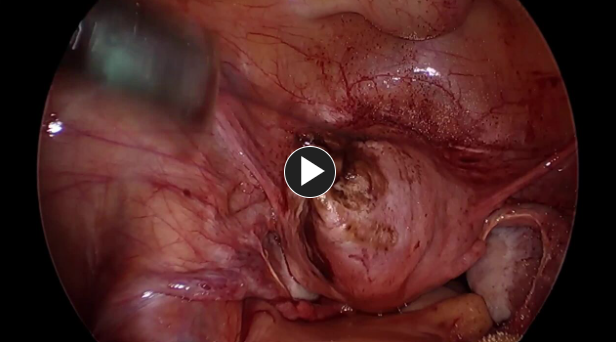
- Use Topical absorbable hemostatic agent such as SURGICEL™ Powder Absorbable Hemostat on the fibroid site for hemostasis as necessary.
- The fibroid is placed in a specimen retrieval bag such as ENDOPOUCH™ RETRIEVER Specimen Bag and is extracted by mini laparotomy.
- Use Topical absorbable hemostatic agent such as SURGICEL SNoW™ Absorbable Hemostat on the suture closure approximation site.

Closure
Closure
- All trocars are removed and a synthetic absorbable suture such as 4-0 Vicryl Plus suture is used to close the trocar sites.
Post-operative Patient Care
Typical recommendations for post-operative care may include, but are not limited to, any of the following:
- Patients should improve each day postoperatively, temperature greater than 38C, and increasing abdominal pelvic pain not relieved by medication should notify their healthcare provider.
- Typical discharge instructions consist of medications for pain management and bowel regularity, diet, and activities, clinic follow-up in 2 weeks.
- Most patients will be discharged the same day or 23 hours stay.
- Patients are recommended to follow any nutritious diet that they can tolerate and generally first try liquids and foods that may be easily digestible.
- Patients are encouraged to ambulate early (with assistance if needed) even on the day of surgery to reduce deep vein thrombosis (DVT) risk.
- Generally, patients are asked to be active as they can tolerate but limit strenuous activities.
Additional resources

Access our on-demand GYN video library
Looking for more? Explore procedural videos and webinars from global experts


