Grace Chen, MD
Total Laparoscopic Hysterectomy

Procedure Overview
A hysterectomy is an operation to remove the uterus. A variety of surgical approaches exist for removal of the uterus, including supracervical hysterectomy, laparoscopic approaches, robot-assisted laparoscopic approaches, total vaginal hysterectomy (TVH), and total abdominal hysterectomy (TAH). Surgeons decide which surgical approach is most appropriate for each individual patient.
INDICATIONS & OBJECTIVES:
A hysterectomy is an operation to remove the uterus. This surgery may be done for different reasons, including, but not limited to:
- Uterine fibroids that cause bothersome pressure, bleeding, or other problems
- Abnormal uterine bleeding
- Uterine prolapse
- Cancer of the uterus, cervix, or ovaries
- Gender affirming care

Relevant Anatomy
Click to interact with a BioDigital Human animated 3D anatomy, disease states, and procedure tour.
Pre-operative Patient Care
Typical recommendations for pre-operative care may include, but are not limited to, any of the following:
- Usually, routine laboratory testing may include a complete blood count, serum electrolytes, age-appropriate health screening studies, and electrocardiogram for women aged 50 years and older.
- Preoperative imaging of the pelvis (MRI, ultrasonography and computed tomography) may be indicated to evaluate the extent of uterine pathology and associated anatomical changes for surgical planning purposes.
Prep & Patient Positioning
Common patient positioning:
- Patients are placed in a dorsal lithotomy position with Allen stirrups and pneumonic compression devices.
- The arms are tucked at the sides and a foam mattress is situated directly under the patient to prevent sliding during steep Trendelenburg.
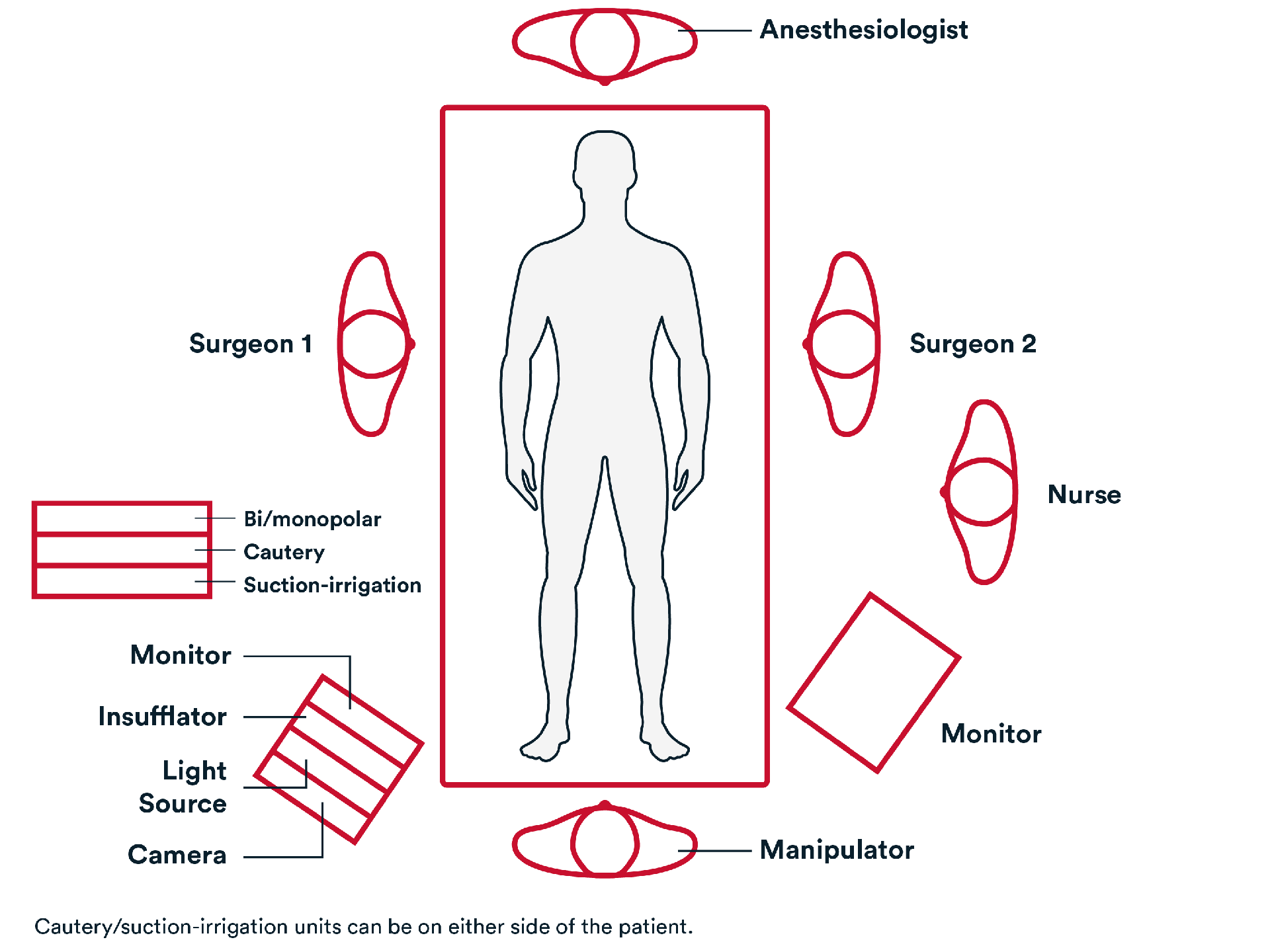
Common port positioning & room setup:
- 5-mm or 10-mm port at the umbilicus for the laparoscope; or Palmer’s point in case pelvic adhesions are suspected to be present.
- 2 bilateral 5-mm or 10-mm ports placed in bilateral lower quadrants, approximately 2 cm medial and cephalad to the anterior superior iliac spine (ASIS), taking care to stay lateral to the inferior epigastric vessels.
- An optional 5-mm port can be placed on either the right or left side, at approximately the level of the umbilicus, along the midclavicular line to avoid the superior epigastric vessels.
Operative Steps

Access
Access
- Access to abdomen is generally gained in one of the 3 ways: Veress needle; direct/optical entry and open entry.
- Anatomic survey is usually performed including pelvic and upper abdomen with particular attention to the course of the pelvic ureters.

- If necessary, adhesiolysis is performed.
Repair
Repair
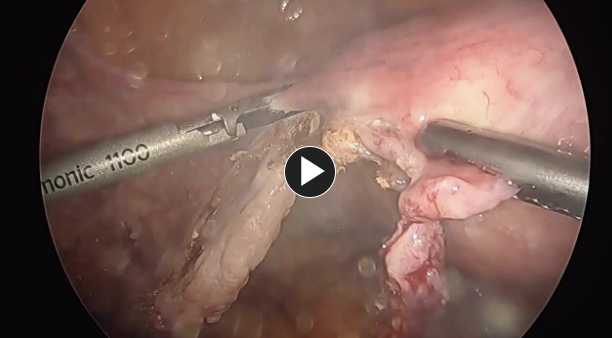
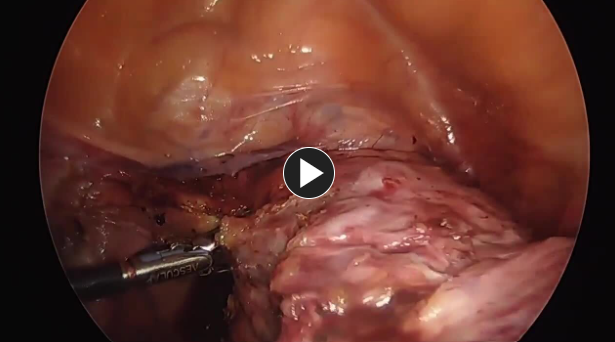
- Round ligaments are ligated and divided using an energy device such as HARMONIC™ 1100 or Enseal ™ X1.
NOTE: to prevent bleeding it may be helpful to divide round ligament at midpoint.
- If fallopian tubes are being removed (conserving ovaries), the mesosalpinx is ligated and divided.
- Utero-ovarian ligaments are transected using an energy device such as HARMONIC™ 1100 or Enseal™ X1.
- If ovaries and fallopian tubes are being conserved, isthmus of fallopian tubes and utero-ovarian ligaments are ligated and divided.
- If ovaries and fallopian tubes are being removed, infundibulopelvic (IP) ligaments are ligated and divided using an energy device such as HARMONIC™ 1100 or Enseal™ X1.
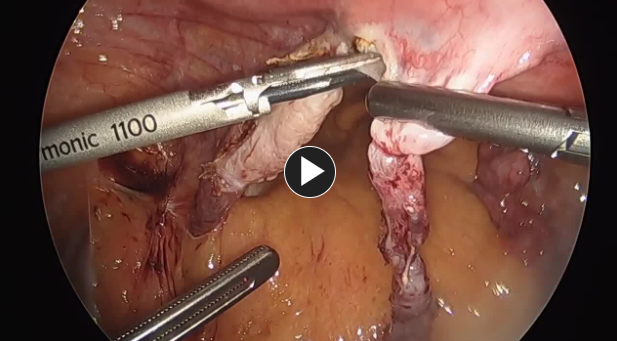
- Broad ligament is incised until uterus reached using an energy device such as HARMONIC™ 1100 or Enseal™ X1.
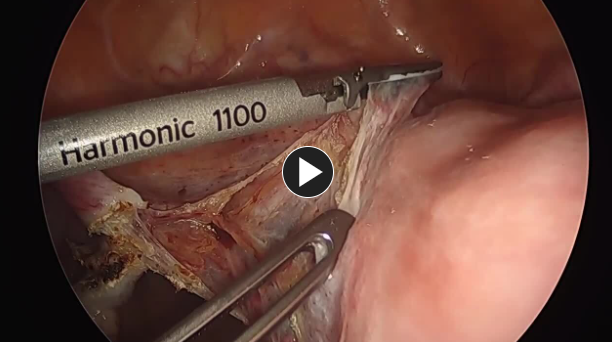
- Anterior and posterior leaf of broad ligament is separated and incised to skeletonize uterine vessel and lateralize ureters using an energy device such as HARMONIC™ 1100 or Enseal™ X1.
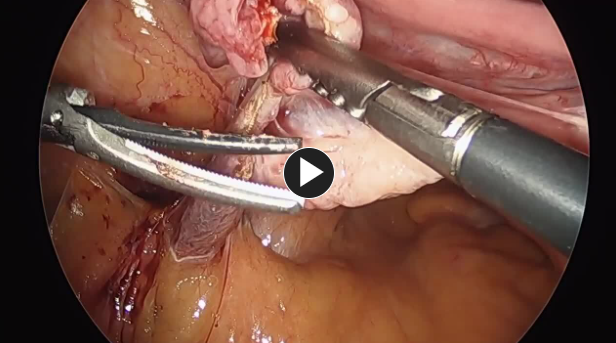
- Vesicouterine peritoneum is incised and bladder dissected away from uterus, cervix and upper vagina (creating the bladder flap) using laparoscopic scissors.
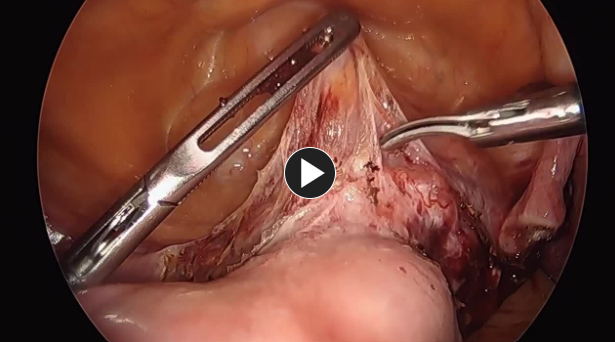
- Uterine artery and vein are skeletonized, ligated, and divided using an energy device such as HARMONIC™ 1100 or Enseal™ X1.
- Cardinal and uterosacral ligaments are divided.
- Colpotomy is performed with an electrocautery hook such as MEGADYNE™ E-Z Clean™ Electrosurgical Electrodes.


Closure
Closure
- Vaginal cuff is closed with an absorbable synthetic suture, like Coated Vicryl® Plus. Antibacterial suture or a knotless tissue control device such as STRATAFIX™ Knotless Tissue Control Device.

- Trocars are removed. The wounds are closed using synthetic absorbable monofilament, such as Monocryl® Plus Antibacterial suture, and a topical skin adhesive such as DERMABOND ™PRINEO™ Skin Closure System or any appropriate dressing.
Post-operative Patient Care
Typical recommendations for post-operative care may include, but are not limited to, any of the following:
- Typical discharge instructions consist of medications for pain management and bowel regularity, diet, and activities (see below), clinic follow-up, and instructions on the signs and symptoms which may indicate potential complications.
- Most patients will be discharged on the same day of surgery especially if Enhanced recovery after surgery (ERAS) protocol is being followed.
- Patients are recommended to follow any nutritious diet that they can tolerate and generally first try liquids and foods that may be easily digestible.
- Patients are encouraged to ambulate early (with assistance if needed) even on the day of surgery to reduce deep vein thrombosis (DVT) risk.
- Generally, patients are asked to be active as they are able to tolerate but limit strenuous activities.
Additional resources

Access our on-demand GYN video library
Looking for more? Explore procedural videos and webinars from global experts

Energy Academy
This program offers concise learning to understand monopolar, bipolar, and ultrasonic energy modalities.