
Christopher Joe Northup, MD
Laparoscopic Sleeve Gastrectomy
Procedure Overview
Laparoscopic sleeve gastrectomy is a surgical weight-loss procedure in which the stomach is generally reduced to about 15-20% of its original size, by surgical removal of the greater curvature of the stomach. Surgical staplers are utilized to perform this resection and the result is a tube-shaped structure. The procedure permanently reduces the size of the stomach and is a restrictive procedure, as well as provides a hormonal impact on a patient’s physiology.
INDICATIONS & OBJECTIVES:
- Sleeve gastrectomy is utilized as a treatment for the disease of obesity and its associated medical conditions.
- According to the ASMBS (American Society of Metabolic and Bariatric Surgery) guidelines for bariatric surgery, the indications for weight loss surgery are as follows:
- BMI equal to or greater than 40
- BMI 35 to 39.9 with one or more related comorbidity including, but not limited to, type 2 diabetes, hypertension, sleep apnea and others.
- BMI 30 to 34.9 with metabolic syndrome or type 2 diabetes

Relevant Anatomy
Click to interact with a BioDigital Human animated 3D anatomy, disease states, and procedure tour.
Pre-operative Patient Care
Typical recommendations for pre-operative care may include, but are not limited to, any of the following:
- Upon entrance to a bariatric surgery program and before proceeding with surgery, patients are generally encouraged to participate in a multidisciplinary program with dietary and lifestyle modifications. This is intended to help ensure the patient is prepared for the necessary behavioral changes for long-term success.
- Based on patients' comorbid conditions, the preoperative evaluation can also involve consultations from a variety of specialists. Often consultants such as cardiologists, pulmonologists and psychologists are a routine part of the workup process.
Prep & Patient Positioning
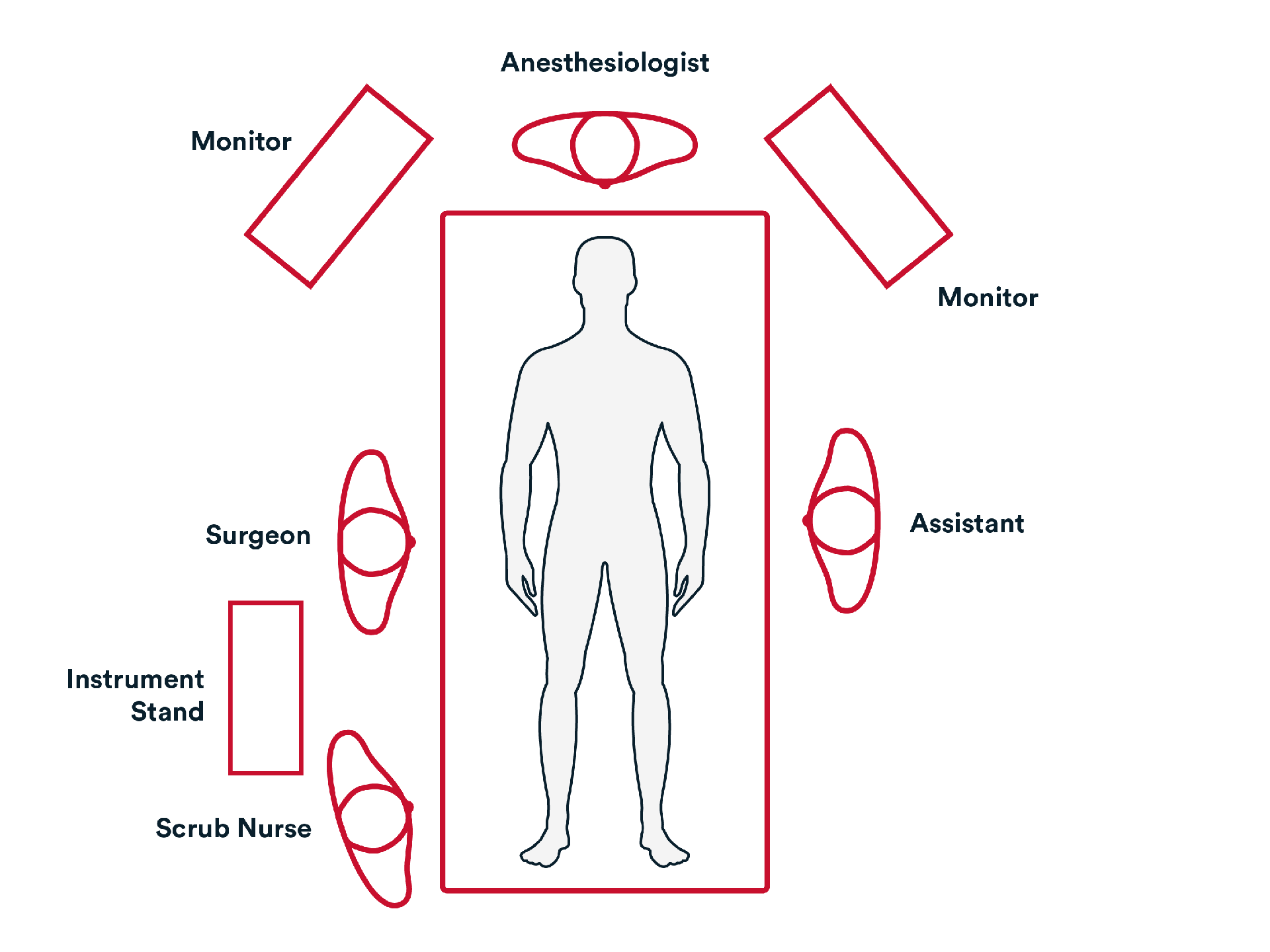
Common patient positioning:
- Typically, the patient is placed in the supine position with arms out laterally.
- Once ports have been inserted, patient is placed in Trendelenburg position.
- The surgeon is usually on the patient’s right side and assistant is opposite.
- Generally, care must be taken with positioning the upper extremities of a patient suffering from morbid obesity as they could be at risk for nerve injury due to their higher BMI.
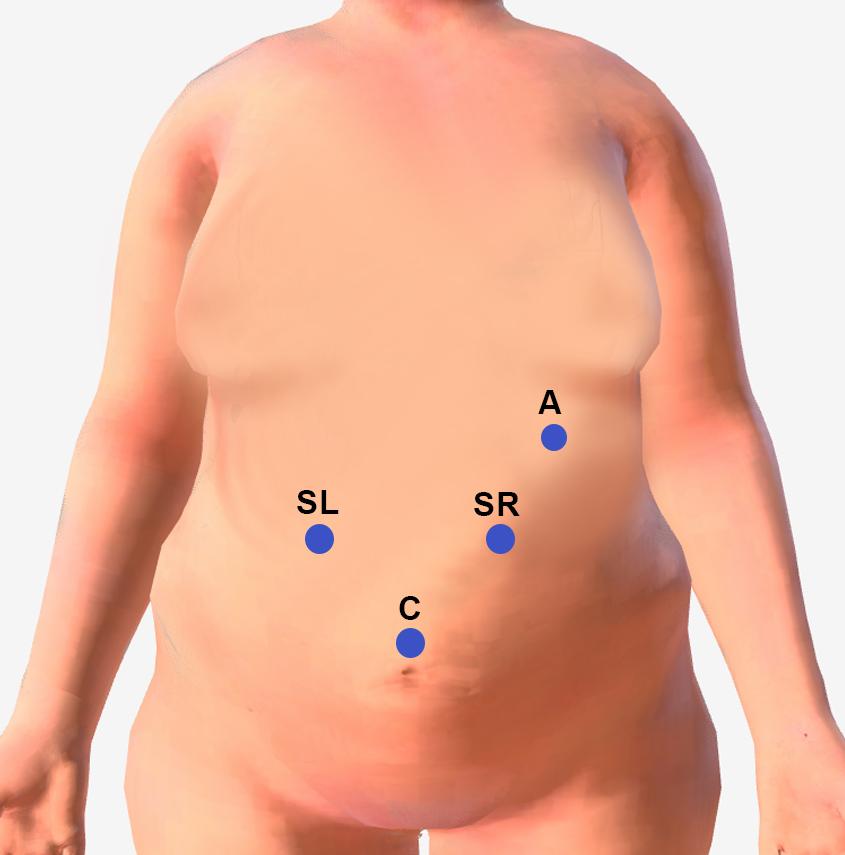
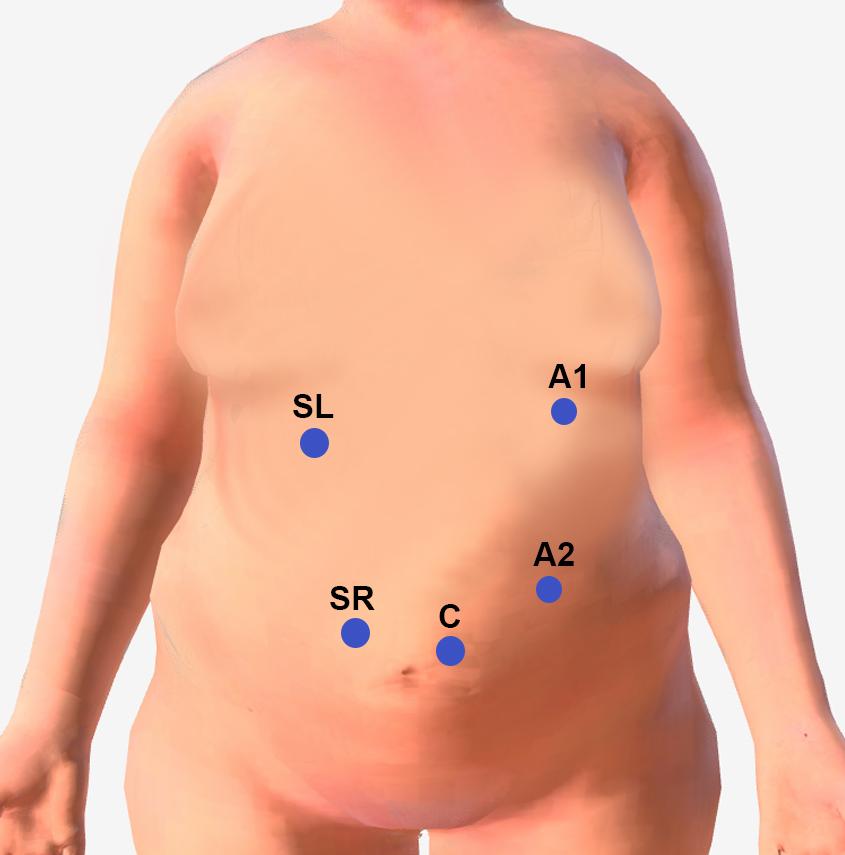
Common port placement: Option 1
- C- Camera
- SR/SL- Operating Trocars- Surgeon Right Hand (SR) and Left Hand (SL)
- A- Assistant Trocars (A1, A2)
- L- Liver Retractor
One trocar site will typically be a 15mm Trocar for extraction of resected stomach.
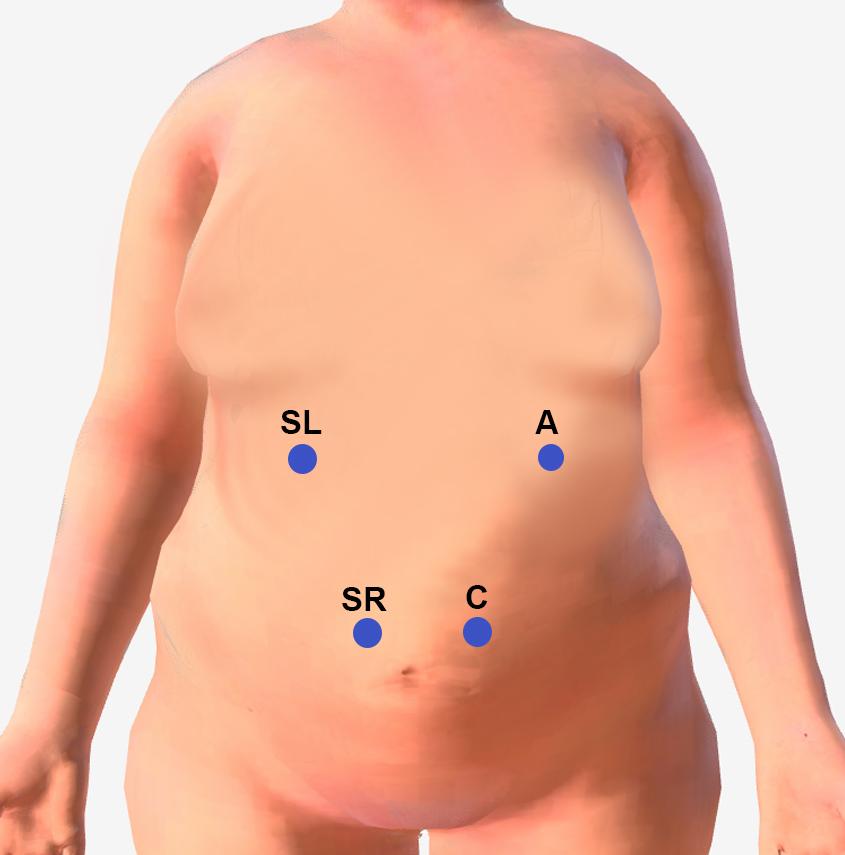
Common port placement: Option 2
- C- Camera
- SR/SL- Operating Trocars- Surgeon Right Hand (SR) and Left Hand (SL)
- A- Assistant Trocars (A1, A2)
- L- Liver Retractor
One trocar site will typically be a 15mm Trocar for extraction of resected stomach.
Common port placement: Option 3
- C- Camera
- SR/SL- Operating Trocars- Surgeon Right Hand (SR) and Left Hand (SL)
- A- Assistant Trocars (A1, A2)
- L- Liver Retractor
One trocar site will typically be a 15mm Trocar for extraction of resected stomach.
Operative Steps

Access
Access
- Trocar sites are identified, and trocars inserted to gain access to the abdominal cavity and stomach. Generally, 4-5 trocars are required.
- Initial Access to the abdomen is generally obtained by either:
- Veress needle technique
- Direct trocar view technique

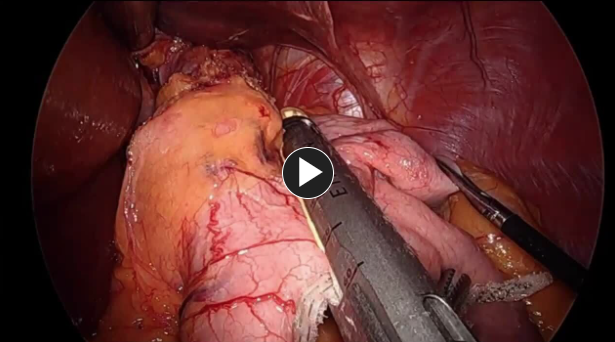
- Upon identifying the Pylorus, the dissection begins at 4-6cm proximal to the Pylorus
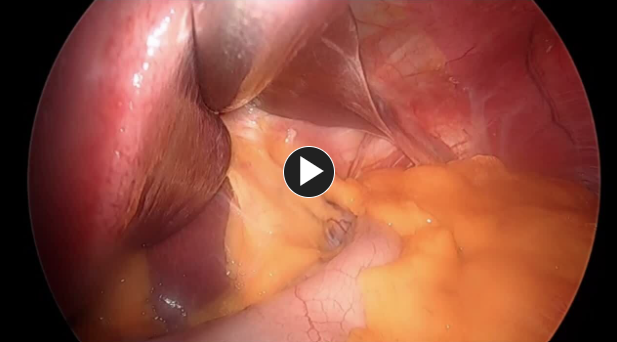
- Attachments to the Greater curvature are mobilized with an energy device such as ENSEAL™ X1 Curved Jaw Tissue Sealer or HARMONIC™ 1100, including the short gastric vessels. The greater curve is mobilized completely to the diaphragm. If an ultrasonic energy device is used, completely encompassing the vessel that is being sealed, and allowing the device time to seal the vessels before lifting against the cutting blade, generally aids in achieving better hemostasis.

Repair
Repair
- A bougie (typically 34-44 Fr) is inserted along the lesser curvature for sizing of the Sleeve pouch.
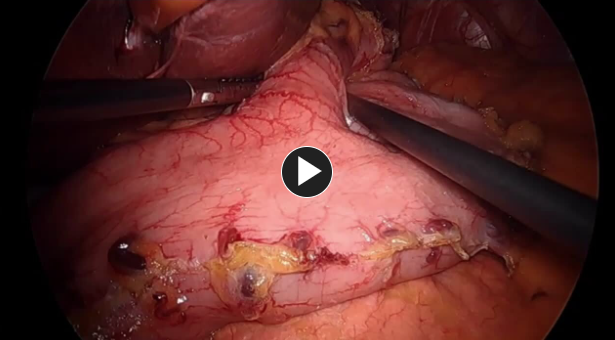
- Sleeve is created using a stapling device such as ECHELON™ 3000 Stapler.
- Generally, the dissection begins 4-6cm from the pylorus.
- Stapler is generally placed at least 2cm from the incisura as stapling too close to the incisura can result in a stricture, severe GERD and increased risk for a more proximal leak.
NOTE:
- The thickness of the stomach typically decreases from distal to proximal. Likewise, there is variability between patients with regard to thickness of the stomach tissue.
- Cartridge selection with different stapling heights to adequately staple the tissue while remaining perfused without oozing can vary based on clinical judgement of stomach thickness.
- Other options including staple line reinforcement (buttress), such as ECHELON ENDOPATH™ Staple Line Reinforcement and oversewing may be utilized depending on surgeon preference.
- Hemostasis along staple line and surgical site can be controlled in many ways if needed. Suturing, clips, or hemostatic agents such as Veraseal™ Fibrin Sealant, are all options to control small areas of oozing.
- A provocative leak test is performed. Leak test can be performed in variety of ways including endoscopy, methylene blue pressure test, air-leak test.


Hiatal Hernia
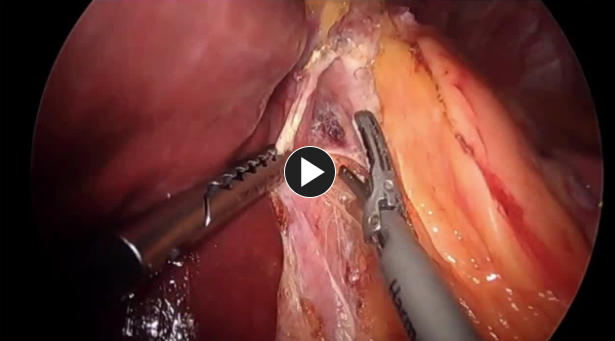
Hiatal Hernia
- A hiatal hernia is a common finding during bariatric surgery. One of the long-term potential complications of a sleeve gastrectomy is GERD. Surgeons are generally prepared for the identification and repair of a hiatal hernia during bariatric procedures.

Closure
Closure
- Specimen is removed through 15mm trocar site.
- Closing the fascia in 15mm trocar defect is generally recommended.
- The intra-abdominal pressure is reduced, and trocar sites observed upon removal to check for bleeding.
- The wounds are closed using synthetic absorbable monofilament, such as Monocryl® Plus Antibacterial suture, and a topical skin adhesive such as DERMABOND PRINEO® Skin Closure System or any appropriate dressing.
Potential complications include but are not limited to:
- Surgical bleeding
- Staple line Leak
- Stricture
- Pseudo-Stricture (narrowing at Incisura, twisting of staple line during creation)
- DVT/ Pulmonary Embolism
- Surgical site infection (deep or superficial)
Post-operative Patient Care
Typical recommendations for post-operative care may include, but are not limited to, any of the following:
- Typical discharge instructions consist of pain management, instructions on the future signs and symptoms indicating potential complications (see below), and an office appointment in 1-2 weeks.
- Most patients will be hospitalized for 23 hours. During that period, patient will be monitored on a surgical unit. They will be given bariatric clear liquid diet, will be ambulatory and encouraged to walk to reduce DVT risk. Chemical and mechanical DVT prophylaxis will be administered. Pain medication as needed. Patient is discharged to self-care at home once the discharge criteria are met.
- Patient will be seen frequently for follow-up. First visit at 1-2 weeks, second at 4-6 weeks, then typically every 3 months until 1-year post-op. Annual visits are expected in addition for long-term follow-up. Support groups are made available in addition to follow up visits. Post op labs may be checked during follow-up to make sure vitamin deficiencies do not develop.
Additional resources

Access our on-demand Bariatric video library
Looking for more? Explore procedural videos and webinars from global experts
Stapling Academy
This program offers interactive learning about the science of stapling and novel stapler design technologies.


